Porphyromonas gingivalis Infection is Associated with Increased Vascular Inflammation in Patients with and Without Coronary Artery Disease
Courtney Levit1, †, Hannah Wheeler1, †, Daniel Sindelar2, Conville Brown3, Nicolas Chronos1 and Marc S. Penn 2, 4,*
1Cardiology Care Clinics, Eatonton, GA, USA
2Keystone Bio, Inc., St. Louis, MO, USA
3The Bahamas Heart Centre, Nassau, Bahamas
4Summa Health Heart and Vascular Institute, Akron, OH, USA
E-mail: marc.s.penn@gmail.com
*Corresponding Authors
†These authors contributed equally to this study
Received 04 March 2024; Accepted 15 March 2024; Publication 20 April 2024
Vascular inflammation is a critical measure of risk for major adverse cardiac events in patients with and without known coronary artery disease. It is recognized that patients with poor oral hygiene tend to have an increased prevalence of coronary artery disease and myocardial infarction. Porphyromonas gingivalis (PG) is the keystone pathogen leading to periodontal disease. Despite evidence suggesting a link between active PG infection and coronary artery disease, there is limited data investigating whether PG can contribute to increased markers of vascular inflammation in patients with coronary artery disease. In this study, we studied 112 consecutive patients who presented at a community preventive cardiology clinic who consented to be assessed for the presence of PG. Subjects were enrolled in a mouth along assessment with measures of vascular inflammation, which was part of their routine clinical care. The average age of patients was 70.4 8.5 years with 48.6% of the patients positive for PG and 20.5% with a history of coronary artery disease (CAD). The distribution of PG positivity was 48.3% and 34.8% in patients without and with a history of CAD, respectively. Patients with CAD have significantly greater levels of high sensitivity C-reactive protein (hsCRP_ (1.3 0.3 vs. 3.2 1.1 mg/dL, p 0.04) and MPO (245.1 19.4 vs. 371.4 39.1 pmol/L, p 0.003). Patients without a history of CAD, only Myeloperoxidase (MPO) was significantly increased. Statin use was significantly greater in those patients with a history of CAD. Interestingly, statin use tended to be greater in PG+ patients (71% vs. 62%) regardless of CAD status. The data from this early study demonstrate a link between active PG infection and increase in markers of vascular inflammation, especially in patients with established CAD. The findings suggest PG as a marker of cardiovascular risk, especially in patients with residual inflammatory risk.
Keywords: Periodontal disease, vascular inflammation, porphyromonas gingivalis, biomarkers, coronary artery disease.
There is growing recognition of the value of inflammatory biomarkers for defining cardiovascular and mortality risk [1, 2]. Recent analyses of lipid lowering studies have shown that residual inflammation identifies patients at increased risk of major adverse cardiovascular events (MACE) despite LDL lowering therapy treatment to less than 70 mg/dL [1, 3]. The fields approach to the excess risk in patients with LDL 70 mg/dL is to further lower LDL. This approach presumes the only drivers of inflammation and residual cardiovascular risk are related to cholesterol.
Proinflammatory conditions have long been linked to cardiovascular risk. Autoimmune diseases like psoriatic arthritis, inflammatory bowel disease and rheumatoid arthritis are all known to significantly increase the risk for coronary artery disease and MACE [4]. Related to the presence of autoimmune diseases or not, the microbiome is increasingly being recognized as mechanism for increased inflammation and coronary artery disease [5]. While significant focus on the microbiome has been in the gut, periodontal disease and the oral microbiome has long been thought increase the risk of coronary artery disease and MACE [6, 7].
A specific keystone pathogen in the mouth is Porphyromonas Gingivalis (PG). There is growing evidence of a link between the presence of PG and several diseases including cancer, Alzheimer’s Disease and coronary artery disease [7–9]. Despite these data, the role of periodontal disease, and more importantly, the potential for prevention and treatment of periodontal disease in patients being assessed for primary and secondary prevention of coronary artery disease is poorly understood. The goal of this study was to determine if the presence of PG is associated with residual inflammatory risk in patients being evaluated at a preventive cardiology clinic for primary and secondary prevention.
This study was approved by the Western IRB, study number 1297875. Consecutive non-smoking patients who presented for care at Cardiology Care Clinic of Lake Oconee were approached to be part of the study. In total, 120 patients were consented. Among these, 112 patients completed the data sets and were therefore included in the analyses.
Medical and dental history along with blood draws for biomarker measurement and paper points for PG assessment were obtained by qualified personnel during the visit. No follow-up was performed. All data were entered into an eCRF to create a locked password protected database from which these analyses were performed. Statistics were performed using Microsoft Excel.
The average age of the subjects recruited to this study was 70 years (Table 1) and most subjects (79.2%) were present for primary prevention without history of CAD. Nearly half (48.6%) of the patients have active PG in the mouth. Table 1 shows 48.3% of subjects without a history of CAD were presented with active PG. This contrasted 34.8% with a history of CAD (p NS). While both genders were equally represented in this study, men were more likely to have a history of CAD than women (p 0.02).
| CAD Neg | CAD Neg | CAD Pos | CAD Pos | ||
| Subjects | PG Neg | PG Pos | PG Neg | PG Pos | |
| Number | 112 | 46 | 43 | 15 | 8 |
| Age (SD) | 70.4 8.5 | 69.8 8.7 | 69.4 8.9 | 75.2 6.0 | 70.0 7.0 |
| % Male | 48.2 | 34.8 | 46.5 | 80 | 75 |
| BMI (SD) | 27.9 5.5 | 27.5 5.1 | 28.5 5.4 | 27.0 7.0 | 28.6 6.3 |
| % T2D | 16 | 13 | 14 | 33 | 12.5 |
The average body mass indices (BMI) of the population was 27.9 which is consistent with the majority being overweight, without a significant difference in BMI whether the subjects had a history of CAD or oral PG. Sixteen percent of subjects had type 2 diabetes. There was an increase in the prevalence of type 2 diabetes in the CAD+/PG- cohort. However, there was no significant difference in the prevalence of type 2 diabetes between those with or without a history of CAD or whether subjects were positive for PG in the mouth.
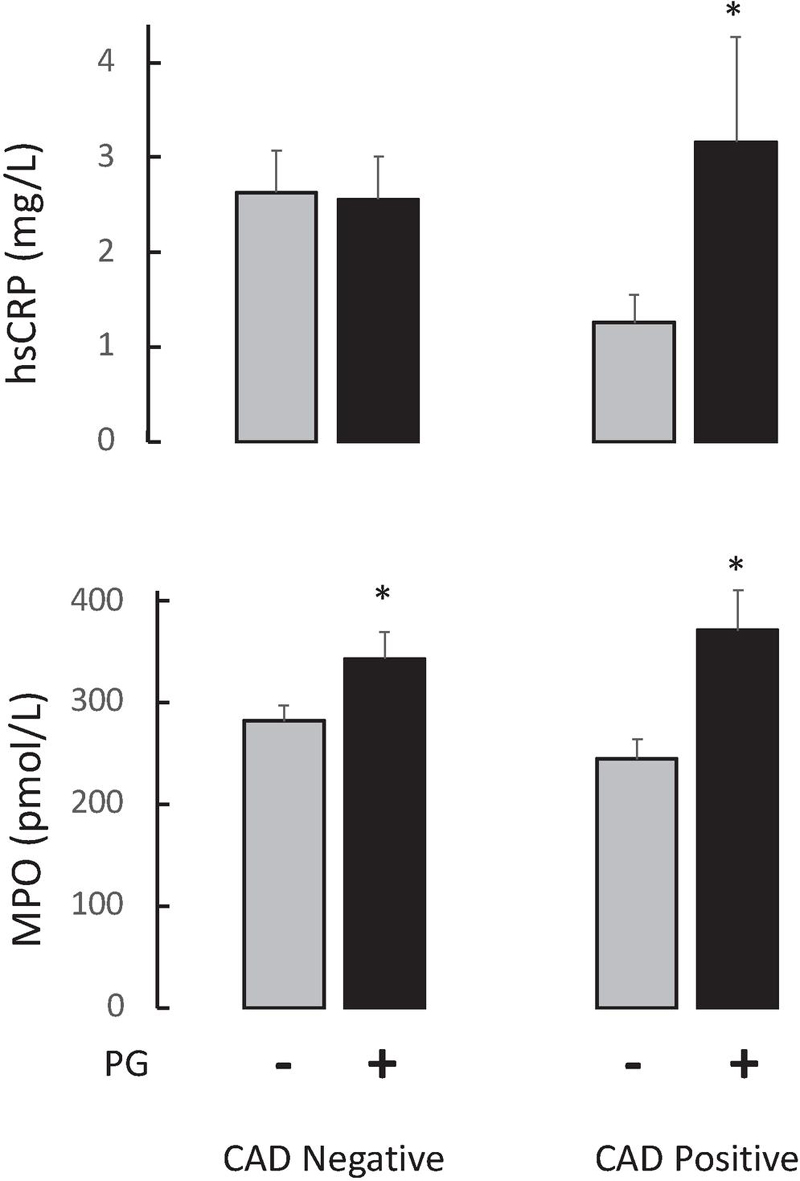
Figure 1 Level of (A) hsCRP and (B) MPO in patients based on whether they had a history of coronary artery disease (CAD) and whether they had active Porphyromonas Gingivalis (PG) infection in their oral cavity. Data represent mean SD. *Identifies an increase in the inflammatory biomarker relative to no PG infection for the same CAD status.
Figure 1 depicts the levels of hsCRP and MPO found in the blood of patients stratified by whether they had a history of CAD or not, and their PG status. These data show that in patients with a history of CAD there was a significant increase in high sensitivity C-reactive protein (hsCRP) in those patients who were PG positive, as compared to those who were PG negative. Interestingly, no statistically significant differences were seen in hsCRP between those who were PG positive or negative in patients with no history of CAD. These data suggest that in patients with CAD, the anti-inflammatory effect of drug therapy, such as statin therapy, is not achieved in the presence of PG.
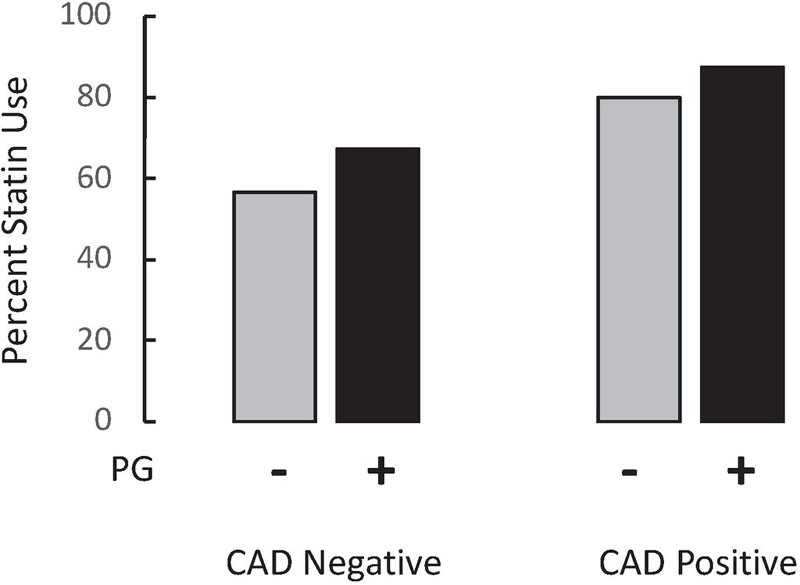
Figure 2 Percent of patients on statin therapy at the time of enrollment based on whether they had a history of coronary artery disease (CAD) and whether they had active Porphyromonas Gingivalis (PG) infection in their oral cavity.
As anticipated, there was greater statin use in patients with a history of CAD compared to those without a history of CAD – 61.8% vs. 82.6% (p 0.049), respectively (Figure 2). There was no significant difference in statin use between those patients with and without PG.
Cardiometabolic risk beyond elevated cholesterol levels is a major driver of the increasing myocardial infarction rate over the last 10 years. The importance of this increased cardiometabolic risk is highlighted by studies that demonstrate the relationship between residual inflammatory risk and major adverse cardiovascular events [1]. Our results indicate that the presence of Porphyromonas Gingivalis could be a significant contributor to residual inflammatory risk as measured by free MPO in the blood of patients with and without a history of CAD. Whereas our data suggests PG only contributes to residual inflammatory risk as measured by hsCRP only in patients with a history of CAD.
Importantly, several mechanisms associated with PG infection in the mouth can lead to increases in systemic inflammation without the need for the bacteria itself to enter the blood stream. Release of lipopolysaccharide, gingipains and fimbriae due to PG in the mouth from the bacteria into the blood stream have been associated with disease states related to inflammation [8]. The recent GAIN trial in patients with mild-moderate Alzheimer’s Disease demonstrated the potential clinical benefit of blocking down-stream pathways of PG that induce inflammation through inhibition of gingipains using a novel small molecule [10]. Interestingly, the benefit was only seen in patients with active PG infections, suggesting quantifying PG infection offers the potential for identifying high risk patients.
PG infection in the mouth of ApoE-/- mice has been shown to increase TMAO levels and atheroma burden [11]. Recently, PG infection in patients with myocardial infarction was shown to be associated with increased levels of TMAO in patients with and without standard risk factors of myocardial infarction [12]. These findings are consistent with our findings and support the concept that PG infection increases the risk of gut dysbiosis, and that identifying the source of inflammation associated with increased cardiovascular risk should include determining whether the patient has on-going PG infection.
This article is part of the journal’s collaboration with The HEALinc, a global future health research and development organization, Bahamas. The subject of this particular article was presented at the 2023 HEALinc Future Health Summit.
[1] Ridker PM, Bhatt DL, Pradhan AD, Glynn RJ, MacFadyen JG, Nissen SE, et al. Inflammation and cholesterol as predictors of cardiovascular events among patients receiving statin therapy: a collaborative analysis of three randomised trials. Lancet. 2023;401:1293–301.
[2] Penn MS, MacRae C, Goldfaden RF, Choksi RR, Smith S, Wrenn D, et al. Association of chronic neutrophil activation with risk of mortality. PloS one. 2023;18:e0288712.
[3] Mohammadnia N, Opstal TSJ, El Messaoudi S, Bax WA, Cornel JH. An Update on Inflammation in Atherosclerosis: How to Effectively Treat Residual Risk. Clinical therapeutics. 2023;45:1055–9.
[4] Durante A, Bronzato S. The increased cardiovascular risk in patients affected by autoimmune diseases: review of the various manifestations. J Clin Med Res. 2015;7:379–84.
[5] Chakaroun RM, Olsson LM, Backhed F. The potential of tailoring the gut microbiome to prevent and treat cardiometabolic disease. Nature Rev Cardiology. 2023;20:217–35.
[6] Ramirez JH, Parra B, Gutierrez S, Arce RM, Jaramillo A, Ariza Y, et al. Biomarkers of cardiovascular disease are increased in untreated chronic periodontitis: a case control study. Aust Dent J. 2014;59:29–36.
[7] Rao A, Kumar BK. Role of periodontal pathogens in atherosclerotic plaque development and progression: An overview. Acta Microbiol Immunol Hung. 2023;70:272–7.
[8] Nara PL, Sindelar D, Penn MS, Potempa J, Griffin WST. Porphyromonas gingivalis Outer Membrane Vesicles as the Major Driver of and Explanation for Neuropathogenesis, the Cholinergic Hypothesis, Iron Dyshomeostasis, and Salivary Lactoferrin in Alzheimer’s Disease. J Alzheimers Dis. 2021;82:1417–50.
[9] Gao S, Zhang Z, Sun K, Li MX, Qi YJ. Upper gastrointestinal tract microbiota with oral origin in relation to oesophageal squamous cell carcinoma. Annals Med. 2023;55:2295401.
[10] Sabbagh MN, Decourt B. COR388 (atuzaginstat): an investigational gingipain inhibitor for the treatment of Alzheimer disease. Expert Opin Investig Drugs. 2022;31:987–93.
[11] Xiao L, Huang L, Zhou X, Zhao D, Wang Y, Min H, et al. Corrigendum: Experimental Periodontitis Deteriorated Atherosclerosis Associated With Trimethylamine N-Oxide Metabolism in Mice. Front Cell Infect Microbiol. 2022;12:919013.
[12] Hernández-Ruiz P, Escalona Montaño AR, Amezcua-Guerra LM, González-Pacheco H, Niccolai E, Amedei A, et al. Potential Association of the Oral Microbiome with Trimethylamine N-Oxide Quantification in Mexican Patients with Myocardial Infarction. Mediators of inflammation. 2024;2024:3985731.
International Journal of Translational Science, Vol. 1, 153–160.
doi: 10.13052/ijts2246-8765.2024.026
© 2024 River Publishers