Celebrating 30 Years in Cardiac Stem Cell Research
Paolo Di Nardo* and Felicia Carotenuto
CIMER-Centro di Ricerca Interdipartimentale di Medicina Rigenerativa, Università degli Studi di Roma “Tor Vergata”, Via Montpellier 1, 00133 Rome, Italy
E-mail: dinardo@uniroma2.it
*Corresponding Author
Received 29 May 2024; Accepted 02 June 2024
Abstract
Thirty years ago, the most prominent cardiovascular scientists gathered in a medieval town near Rome to scrutinize the actual possibility of regenerating the myocardium. They agreed to the vision, but the knowledge and technology available were not mature to allow the development of clinically suitable protocols for regenerating the post-ischemic cardiac muscle. Subsequent intensive efforts of thousand scientists and exorbitant investments worldwide have generated many progresses without unraveling the complexity of using healthy cells or fabricating stripes of engineered tissue to be implanted in injured hearts. However, even if the final goal appears not yet at hand, the lesson learned brings us much closer to efficient protocols for clinical use.
Keywords: Cardiac cell therapy, cardiac regeneration, tissue engineering, induced pluripotent stem cell, stem cell therapy, myocardial infarction.
Brief Introduction
Across the centuries, the regeneration of organs and bodies has charmed the mankind under different civilizations and beliefs. Lizards and salamanders may shed their tails and legs and, then, regenerate them. The liver can regenerate if injured, suggesting to our ancestors the myth of Prometheus and the fire, and inspiring the haruspexes (seers practicing divination by inspecting entrails). However, in the last century, it has been possible to ascertain that different animal species and their tissues display a specific regenerative potential [1]. The regeneration of the tissues was attributed to the capability of the somatic cells to de-differentiate and, then, divide and finally differentiate to restore the tissue gap determined by the injury [2]. Among them is the mammalian skeletal muscle, but not the myocardium, in which the division and proliferation of terminally differentiated contractile cells is missed and cannot repair the tissue injured after the myocardial ischemia [3]. To discuss about this peculiar characteristic of the heart muscle, all the most important scientists working on this specific topic were invited to meet in Viterbo (a medieval town near Rome), in the room where nine centuries ago the first conclave was summoned to elect a pope [4].
Cardiac Regeneration – Rationale and History
In 1994, we formed a scientific conclave (Viterbo meeting) to thoroughly discuss the regenerative potential of the myocardium (Figure 1). This 5-day forum also discussed future research directions envisioned to develop innovative technologies to use healthy cells to repair the myocardial damage in the clinical setting. The final goal was determined to substitute post-ischemic injured cells to restore cardiac function and suppress dangerous arrhythmias. The turning point in this narrative occurred in the early 2000s, when stem cells were identified in different tissues, including the myocardium [5]. These tissue-specific stem cells represent the strategic reservoir of cells for tissue repair. More importantly, the stem cells are hosted in particular loci (niche) that can be activated to induce differentiation when needed to repair tissue damage. Regrettably, the myocardium hosts a meager number of stem cells, not sufficient to repair a post-ischemic damage. In order to use the cardiac stem cells in the clinical setting for cardiac repair, it was necessary to preliminarily expand in culture, induce to differentiate, and, then, implant them into the myocardium [6, 7]. This new direction has fueled research worldwide. It should be noted that many investigators involved in stem cell research participated in the Viterbo meeting. This was evident by the wealth of papers published in the following years. PubMed search with “cardiac stem cells” shows that a very few papers were published until 1999 and circa 30000 in the interval 2000–2023, without considering other dozen connected papers, e.g. on the relationship stem cell-ECM (Figure 2).
Figure 1
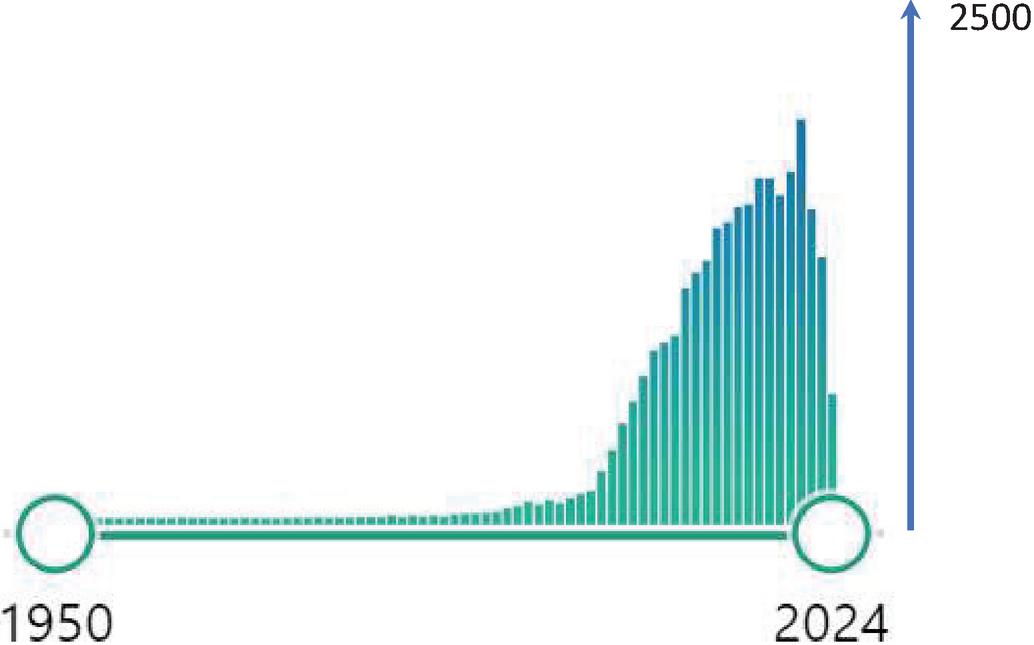
Figure 2
Promise
The massive amount of data generated has represented an invaluable contribution to the knowledge of stem cells biology and their potential. However, the main goal of treating cardiac diseases with healthy cells has been missed, so far, despite an impressive amount of grants invested worldwide. This failure has many causes, among which it can be mentioned the lack of standardization of materials and procedures in face of an extensive marketing of unproven, inconsistent and uncontrolled treatments proposed to patients with severe cardiac diseases. The idea that has been ‘sold’ to patients and their families has been that a simple injection of suspended cells arbitrarily dubbed “stem cells” on the basis of variegated criteria could miraculously determine the repair, if not the restitutio ad integrum, of tissues hit by different diseases or trauma [8]. The concept is analogous to the Gold Rush in which the possibility to mine gold unleashed a foolish competition, the possibility that stem cells could repair injuries in all tissues by a simple cell injection induced many scientists to irrationally compete in the hope to patent their own procedures and become billionaire.
Evolving Experimental Approach
In recent years, new hope was offered with induced pluripotent stem cells (iPSCs) obtained from somatic cells. iPSCs that can propagate indefinitely and ideally differentiate in all types of somatic cells, including cardiomyocytes [9, 10]. A few controlled clinical trials are ongoing, although iPS generation still suffers from low efficiency, risk of tumorigenicity, mutations, and incomplete reprogramming [11]. However, the need to find an optimal cell source has diverted the attention from other crucial issues.
Myocardium displays a 3D anisotropy, baffling biomechanical properties, and a complicated micro/nano bio-architecture. Furthermore, cardiomyocytes display a very peculiar distribution of gap-junctions and capability to regulate electroconductivity. Cardiac cells produce their own extracellular matrix (ECM). However, during the initial stage of their implantation the lack of specific ECM hampers cell survival. Finally, the implanted healthy cells should survive and differentiate in or around an ischemic area in which key parameters are severely altered. These include tissue pH, O tension, cytokine concentration, and cell debris [6]. There are no reliable indications on how these hurdles could be overwhelmed or circumvented. Investigators are mostly focused on defining the intracellular mechanisms of stem cells while neglecting to consider extracellular factors that allow cells to survive, differentiate and incorporate in the hosting tissue. In fact, few cells survive after implantation with insignificant contribution to improve cardiac function. Inconsistent results have also been obtained seeding stem cells on biocompatible scaffolds emulating the ECM to fabricate strips of tissue to be implanted in the ischemic area. Also, in this case, many issues remain unresolved; among many others, the proper design of 3D scaffolds is preliminary to any attempt that grows and differentiate new contractile cells. In fact, the 3D scaffolds are fundamental to mimic the structural complexity of the native cardiac tissue microenvironment providing functional and three-dimensional (3D) support, and promoting targeted regeneration of the damaged myocardium [12]. Engineered 3D tissues also require a suitable functional vascular network to provide the new tissue with adequate blood supply and waste removal.
Cardiovascular diseases are the most lethal killer of mankind. Stunning improvements in their management and treatment have been achieved over the last decades; nevertheless, current cardiac therapy remains palliative and strategies able to cure myocardial injuries and their consequences on the cardiac function are not yet at hand. The 1994 conclave has shifted the paradigm envisioning a novel scenario to treat severely ill cardiac patients [4]. Thirty years of intensive research worldwide has demonstrated the feasibility of novel treatments substituting damage with healthy cells. However, the results so far achieved are not yet “clinical grade”. Actually, the technology needed to repair tissues using cells (floating or as engineered tissue) is at the highest level of complexity. To tackle the intricacy, we must learn from the past thirty years and finally agree a choral effort involving all the major research centers worldwide. This will benefit science, but, above all, patients without reliable alternatives. The spirit of Viterbo 1994 is still alive.
Acknowledgment
We acknowledge the New York Academy of Sciences for permission to reproduce this cover image.
References
[1] Ausoni, S.; Sartore, S. From Fish to Amphibians to Mammals: In Search of Novel Strategies to Optimize Cardiac Regeneration. J Cell Biol. 2009, 184: 357–364.
[2] Kolios, G.; Moodley, Y. Introduction to Stem Cells and Regenerative Medicine. Respiration. 2012, 85: 3–10.
[3] Senyo S.E., Steinhauser M.L., Pizzimenti C.L., et al. Mammalian heart renewal by pre-existing cardiomyocytes. Nature. 2013; 493:433–436.
[4] Claycomb W.C., Di Nardo P. Cardiac Growth and Regeneration. Annals of the New York Academy of Sciences. Volume 752. NY Acad Sci. 1996.
[5] Nadal-Ginard, B.; Kajstura, J.; Leri, A.; Anversa, P. Myocyte Death, Growth, and Regeneration in Cardiac Hypertrophy and Failure. Circulation Research. 2003, 92: 139–150.
[6] Carotenuto, F.; Teodori, L.; Maccari, A.M.; Delbono, L.; Orlando, G.; Di Nardo, P. Turning Regenerative Technologies into Treatment to Repair Myocardial Injuries. J Cellular Mol Med. 2020, 24: 2704–2716.
[7] Carotenuto, F.; Manzari, V.; Di Nardo, P. Cardiac Regeneration: The Heart of the Issue. Curr Transpl Rep. 2021, 8: 67–75.
[8] Eschenhagen, T.; Bolli, R.; Braun, T.; Field, L.J.; Fleischmann, B.K.; Frisén, J.; Giacca, M.; Hare, J.M.; Houser, S.; Lee, R.T.; et al. Cardiomyocyte Regeneration. Circulation. 2017, 136: 680–686.
[9] Takahashi, K.; Yamanaka, S. Induction of Pluripotent Stem Cells from Mouse Embryonic and Adult Fibroblast Cultures by Defined Factors. Cell. 2006, 126: 663–676.
[10] Takahashi, K.; Yamanaka, S. Induced Pluripotent Stem Cells in Medicine and Biology. Development. 2013, 140: 2457–2461.
[11] Youssef, A.A.; Ross, E.G.; Bolli, R.; Pepine, C.J.; Leeper, N.J.; Yang, P.C. The Promise and Challenge of Induced Pluripotent Stem Cells for Cardiovascular Applications. JACC Basic to Transl Sci. 2016, 1: 510–523.
[12] Weinberger, F.; Eschenhagen, T. Cardiac Regeneration: New Hope for an Old Dream. Annual Rev Physiol. 2021, 83: 59–81.
International Journal of Translational Science, Vol. 1, 161–166.
doi: 10.13052/ijts2246-8765.2024.031
© 2024 River Publishers