Mauritius eHealth – Trust in the Healthcare Revolution
Leckraj Amal Bholah1,* and Kemley Beharee2
- 1University of Edinburgh, United Kingdom
- 2University of Mauritius, Mauritius
Corresponding Author: drbholah@gmail.com
Received 5 March 2016;
Accepted 24 May 2016
Abstract
The aim of eHealth infrastructure is to harness innovations in digital infrastructure that can enable the seamless access to, sharing and reuse of data (e.g. clinical records, genomic data and images) irrespective of source [1]. eInfrastructure is comprised of networked, interoperable, service-oriented, scalable computational tools and services. The key element is the interaction of human users and computers so as to facilitate discovery, linking and reasoning [2].
Keywords
- Mauritius
- eHealth
- mHealth
- Doctor Assistant
- Africa Health
- Innovation
- Medical
- Information
- eInfrastructure
- Big Data
- Health Informatics
- Global eHealth
1 Introduction
During the 1990s, as the Internet gained public attention, a number of e-terms began to appear and proliferate. The introduction of eHealth represented a promise of information and communication technologies to improve health and the healthcare system [3]. eHealth infrastructures are viewed as central to the future provision of safe, efficient, high quality, citizen-centered health care. While Western countries have raced forward in developing eHealth, many developing countries remain on the start line. There is evidence that better tapping ICT (Information Communication Technology) could result in more effective utilization of health services and increased efficiency [4]. A communication revolution is brewing in the delivery of health care and the promotion of health fueled by the growth of powerful new health information technologies [5]. Mauritius has one of the most successful and competitive economies in Africa; 2008 GDP at market prices was estimated at $8.128 billion (official exchange rate) and per capita income at $12,100 (purchasing power parity), one of the highest in Africa [6].
2 Mauritius eHealth Potential
Mauritius has a population of 1.2 million residents. There are five regional hospitals and two district hospitals. The number of beds in government health institutions was 3,581 at the end of 2013. In the private sector, there were seventeen private health institutions with a total of 690 beds. The total number of beds in the public and private sectors at the end of 2013 was thus 4271, that is, 285 inhabitants per bed. In 2013, a total of 5.2 million cases was seen by doctors at the out-patient service points in the public sector [7]. There is a need to extend healthcare services beyond medical premises. Despite being built for acute events, many hospitals allot a significant number of their beds to chronically ill patients, with considerable cost consequences. Mobile penetration rate was around 82% in 2009, paving way for intense competition among operators to retain their customers and acquire new ones. Today, mobile penetration is nearly 100%. HSPA (High Speed Packet Access) and EV-DO (Evolution Data Optimized) based 3G services are competing with fixed-line DSL (Digital Subscriber Line) and other wireless broadband offering, including WIMAX (Worldwide Interoperability for Microwave Access) [8]. Efficient remote monitoring and care has a great potential. Adopting a proper eHealth infrastructure can strengthen our health systems by:
- Improving the availability, quality and use of information and evidence through strengthened health information systems and public health surveillance systems.
- Developing the health workforce and improving performance by eliminating distance and time barriers through telemedicine and continuing medical education.
- Improving access to existing global and local health information and knowledge.
- Fostering positive lifestyle changes to prevent and control common diseases.
The Mauritian Government seeks to enhance prosperity for its citizens and to ensure that it is available to everybody, to develop the island further in order to compete with other states in a globalized world and to expand and cultivate the welfare and education systems to promote de facto equal opportunity, regardless of gender, ethnicity, social class or religion. This is the case too in terms of Mauritius ICT policy and strategies where a holistic approach has led to successive policies aimed at ensuring that ICTs contribute to the wealth and prosperity of the country [9].
Since 1989, Mauritius has been a front-runner in an overall comprehensive national ICT policy and liberalized telecommunications framework, more recently in line with the Millennium Development Goal (MDG) [10]. Despite all the opportunities that Mauritius have compared to other African country, a proper eHealth infrastructure has failed to be set up. Major barriers for successful implementation are [11]:
- Limited Awareness of eHealth
Policy makers, health authorities and health practitioners are not fully aware of the potential benefits of the use of ICT for health. The long-term strategic plans for developing eHealth infrastructure is limited.
- Lack of an enabling policy environment
National policies, strategies or regulatory framework are necessary for establishing common technical infrastructure, interoperability and standardization protocols. Mauritius also needs to address ownership, confidentiality, security of data and quality of information.
- Weak leadership and coordination
The challenge is to strengthen coordination and collaboration among stakeholders, partners and donors as well as improve the capacity of the health sector to lead the process.
- Inadequate human capacity to plan and apply eHealth solutions
Number of health workers capable of leveraging ICT in their work remains limited. Health workers are not systematically trained in use of ICT. Mauritius needs health workers with the capacity to design, deploy and effectively manage eHealth projects.
- Weak ICT infrastructure and services within the health sector
Ministries in charge of communications, technology and finance are primarily responsible for national ICT infrastructures. eHealth requires a dedicated team to sustain eHealth initiatives.
- Inadequate financial resources
Collaboration and coordination between multiple partners from both private and public sectors is required.
Despite these challenges, opportunities exist for planning and deploying eHealth solutions. These include the rapid advances in ICT, increasing access to mobile phones and broadband connectivity, increasing interest by donors and countries in strengthening health systems, and the partnerships being built by agencies such as WHO, International Telecommunications Union (ITU), World Bank, United Nations Economic Commission for Africa and others. These partnerships seek to develop national road maps for eHealth, and provide access to a suite of eHealth applications and solutions for enhancing professional capacity. Policy makers should see the eHealth change as innovative, new and valuable. eHealth innovations can gain momentum and acceptance rapidly in the Mauritian society [12].
“We have beautiful hotels, beautiful beaches, and first-class service. Why not make Mauritius a hub, a place where people can combine a holiday and medical treatment” (Former Minister of Health) [13].
“Involve the user” is a mantra in IT development, yet numerous projects fail (some sources report 70% failure [14]) because of inability to capture user insights. It is attributable to failure on the part of developers to understand the workflow of health professionals and to meaningfully involve users in the design, development and implementation [15]. There is also resistance from clinicians who perceive the project as an effort to introduce technology for ‘policing’ their clinical practice. A possible solution for this resistance, is to spend time and energy into building a rapport with clinicians through informal chats, gatherings and social activities.
eHealth infrastructure should support clinician and researcher in time-consuming evaluation tasks to get meaningful results faster and with less effort [16]. Data protection is a major issue which eHealth has to address. It is easy to being stuck in an endless “yes-no” debate regarding Data protection. An interesting solution to the problem is pseudonymisation which means de-identification of medical data [17]. Beside protecting identity of persons and legal entities, systems also need to be protected. This goes as well for molecules (e.g. in drug discovery projects where pharmaceutical research institutes have a need to share basic research information, without exposing intellectual property details).
Patients are now taking responsibility of their own health, receiving information about health matters, and participating in decision making related to personal health issues from prevention to care and follow up [18]. The application of Big Data into eHealth systems will generate a new era of evidence-based medicine.
3 mHealth
mHealth interventions is on the rise. There is no ideal way of deploying mobile technology. Learning from early mHealth deployments is important so that ineffective approaches are not duplicated. Successful projects need to be replicated and scaled. In each mHealth thematic area, the challenges, barriers, and gaps in mHealth manifest themselves in unique and interrelated ways both in LMIC (Low and Middle Income Countries) as well as in high-income countries [19]. A general observation is that mHealth interventions in high income countries focus on chronic diseases while in LMIC on infectious diseases mostly. In high income countries, mHealth addresses mostly the following health conditions according to a Global health report in 2006 [20]:
- Diabetes (blood sugar monitoring)
- Breast cancer (telephone counseling)
- Tuberculosis (adherence to medication)
- Attendance to health facility appointments
- Depression outcomes
- Immunization rates
- Asthma management
- Smoking cessation
Mobile technology plays an empowering role for patients. They feel to have control over their health. The text messaging support system “Sweet talk” was evaluated by Franklin, Greene, Waller and Pagliari. C for its effectiveness in encouraging good diabetes management in young people. The randomized controlled trial (RCT) consisted of sixty-four young diabetes patients. The study concluded that “Sweet talk” effectively engaged young people in self-management of diabetes [21]. Compared to traditional paper and pen methods mobile technologies provide several benefits namely:
- Improved accuracy
- Reduction in time
- Reduction in human resources
- Reduction in cost
- Improved data quality
- Potential for real time authentication of data
- Less interviewer bias
In a paper entitled “Catalysing a perfect storm”, the authors describe how mobile phones are equipping populations with a convenient tool to become better informed, motivated and self-managed to integrate more healthful daily activities [22]. Medic Mobile has been described as Weapon Number one for the war against AIDS [23]. Medic Mobile developed an open source software which is a web-application for sending and receiving messages as well as scheduling time-targeted confirmation notes to conventional $10 mobile phones. A parallel SIM transforms inexpensive mobile phone into a sophisticated wireless data collection terminal. Once the parallel SIM is installed beneath a carrier’s normal SIM card, the software allows for wireless data collection in remote or Internet inaccessible locations (Medic Mobile, “Impact,” 2012).
The Ebola epidemic is a major recent crisis. International collaboration has a crucial role in tackling epidemic. The technology company IBM launched a disease-mapping system in October 2014. AirTel and IBM collaboration allowed local people to send free text messages about Ebola to the Government. Heat-maps that link emerging issues to location information were created [24]. In Sierra Leone, the Red Cross has worked in collaboration with AirTel to launch a platform to send informative text messages to people in most affected areas. 2 million people are thought to have been reached via this platform with messages encouraging simple hygiene measures such as regular hand washing and appropriate personal protective equipment when taking care of ill patients at home [25]. This clearly shows the role of mHealth interventions as both preventive and educational. The spread of cholera after 2012 earthquake in Haiti has been mapped by tracking population movements via mobile phone [26]. The Humanitarian OpenStreetMap Team (HOT), an NGO (Non-Governmental Organisation) that works, train, coordinate and organize mapping on OpenStreetMap for humanitarian, disaster response and economic development has mobilized volunteers from around the world to help map since the Haiti earthquake. In the recent Nepal earthquakes, more than 4300 mappers have made 86 000 edits to map, adding up to 30 000 roads and 240 000 building [27]. Imagine mapping all phone signals in a particular devastated area and this helping rescuers to allocate resources to organize help. Mobile phones can actually save lives and an appropriate disaster management plan using mobile phone resources contributes to disaster preparedness of the country. SMS is an effective strategy to raise fund during recovery phase of a disaster. 27 million Euros have been raised for the United Nations Children’s Fund (UNICEF) in Italy after the tsunami in December 2004 [28].
However, mHealth interventions face many barriers namely:
- Lack of data security
- Difficulties for users in finding the right mHealth solutions
- Devices do not meet clinical requirements e.g. hygiene
- Lack of standardization
- Missing or unknown legitimacy of mHealth publishers
- Mismatch of target group and smartphone owners (elderly/chronic disease)
- Missing regulations
- Patient’s discomfort with change in their healthcare routine
- Lack of profitable business models
- Resistance from traditional healthcare providers
- Lack of high quality clinical studies
- Lack of reimbursement for mHealth apps from company funds and insurance
- Lack of interoperability of mHealth app-based solutions
- Lack of high quality mHealth apps
The demand for wearables is on the rise namely with Apple Watch and Samsung Gear. Soon, there will be an overflow of patient data. The tsunami of information presents a challenge for summarizing all data into usable and meaningful format. In Mauritius, a patient Electronic Health Record (EHR) can be used to collect data, follow up on treatment compliance and draft disease management programs on a national as well as an individual basis. The shift toward integrated mHealth intervention is a new strategy for healthcare providers to adopt technology.
4 Mauritius eHealth Start-up
A survey conducted in Mauritius by the authors, disclosed that, according to patients, doctors have limited time to communicate with them. Furthermore, the waiting time in hospitals is increasing. In several cases, hospitals are perceived by patients to be disorganised. Many patients that were interviewed said that they are frustrated when Doctors ask them the same questions repeatedly. It has also been observed that patients have reported that they have not been well informed about drug usage and follow ups. Patients are unhappy that their medical folders are not transferred across hospitals and when it is done among some hospitals, the folders get lost all too often in the process. They also complain that their blood results also get lost often in the hospital and it is depressing to have blood samples withdrawn several times.
According to patients the above points constitute the main causes of medical negligence. Moreover the survey disclosed that 66% of patients believe that the current health system is the source of the problem. The issue of medical negligence is further accentuated by poor communication between patients and doctors. The authors later developed Doctor Assistant which is a free Electronic Medical Record (EMR) application available for free from Google Play [29]. The application is now being used by 2240 users worldwide and bears a rating of 4.6 upon 5 among medical apps on Google play (Figure 1). Doctor Assistant will be published in the WHO Compendium of Innovative Health Technologies 2014–2015. See annexed illustrations regarding Doctor Assistant features. The project has been taken up by the Mauritius Research Council and State Informatics Limited for further development and the main aims of the final software will be.
- Development of a National Healthcare Information System (patient-centered) for Mauritius and for the region, to improve health services in public and private hospitals, as well as for private practitioners.
- Provide a common robust and scalable platform to stakeholders of the medical sector, which will enable global visibility on issues and trends, and contribute to an early health warning system through timely access and secured sharing of medical information (Smart Data, Big Data, Data mining, Open Data).
- Conceive a user interface which is adapted and customised for the healthcare sector, with features to minimise human errors and mitigate cognitive overload (Figure 2).
- Enable self-monitoring of patient in real-time of his/her health status and treatment history.
- Support and improve diagnosis and decision making through the use of intelligent algorithms and techniques (out-patient and casualty).
- Make full use of mobile, tablet and cloud technologies to support above objectives (Figures 3–6).
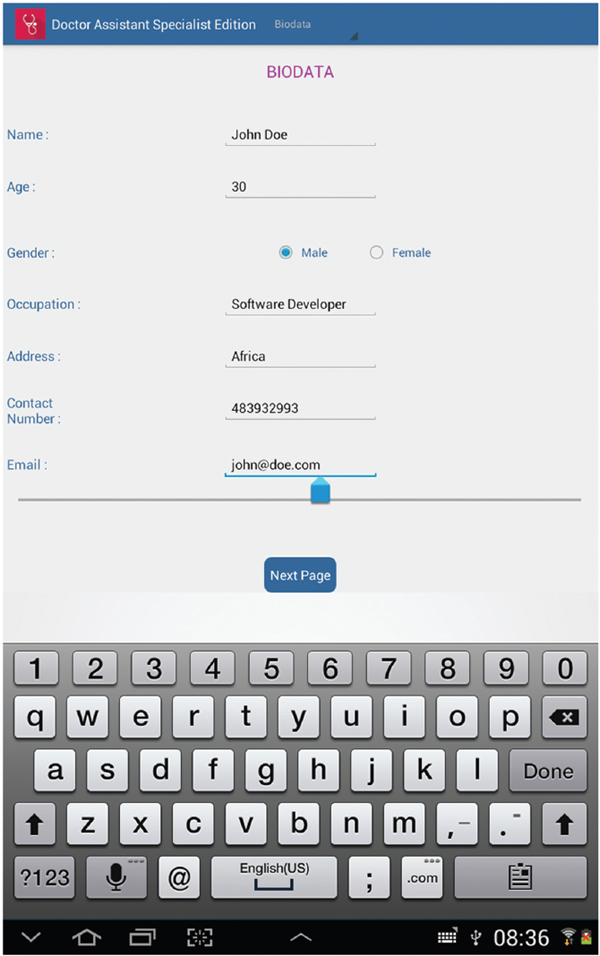
Figure 1 The Biodata template provides a practical and easily fits clinician’s daily use.
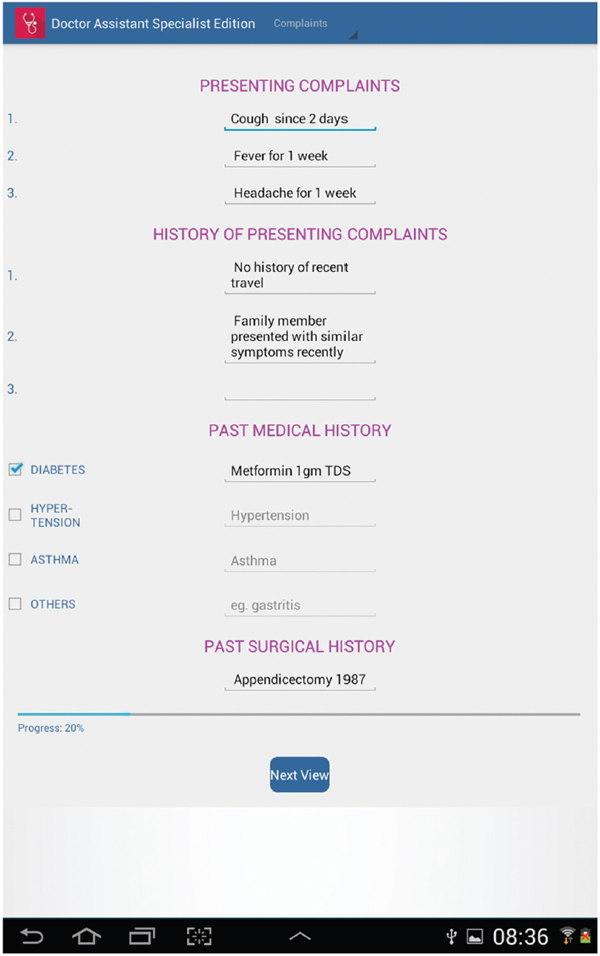
Figure 2 Medical template helps clinicians reduce medical errors.
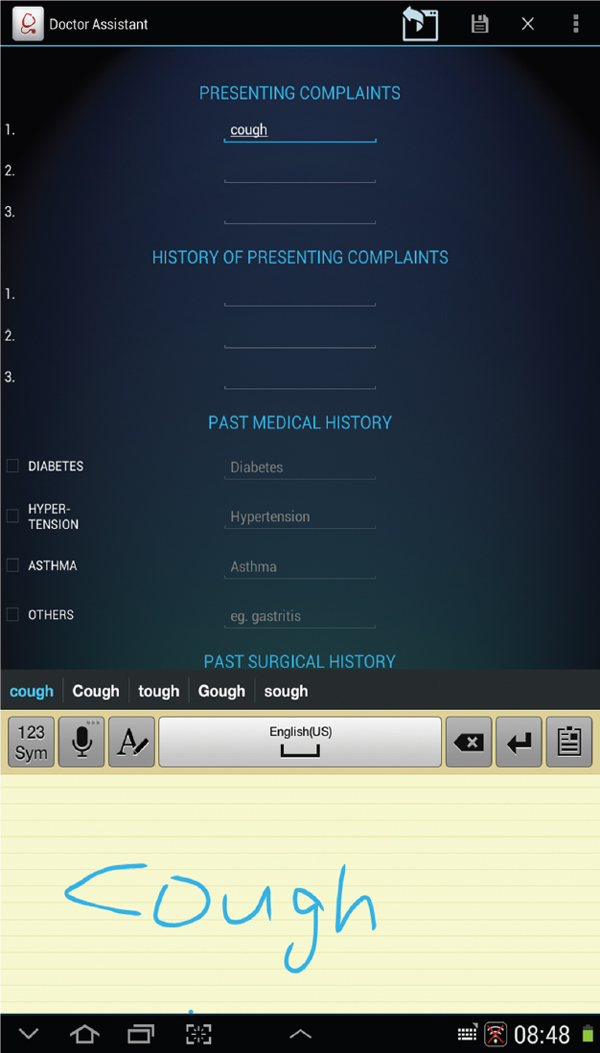
Figure 3 Handwriting recognition is an integral part of the EMR thus facilitating the task of clinicians.
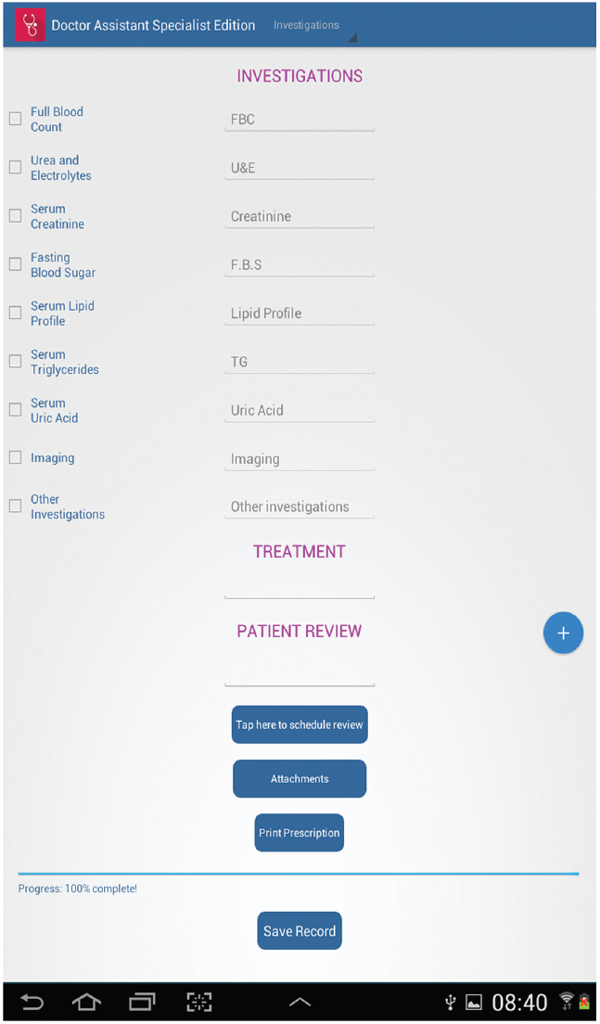
Figure 4 The final page of the consultation process allows the clinician to schedule an appointment, add attachments and print the prescription using Cloud printing services.
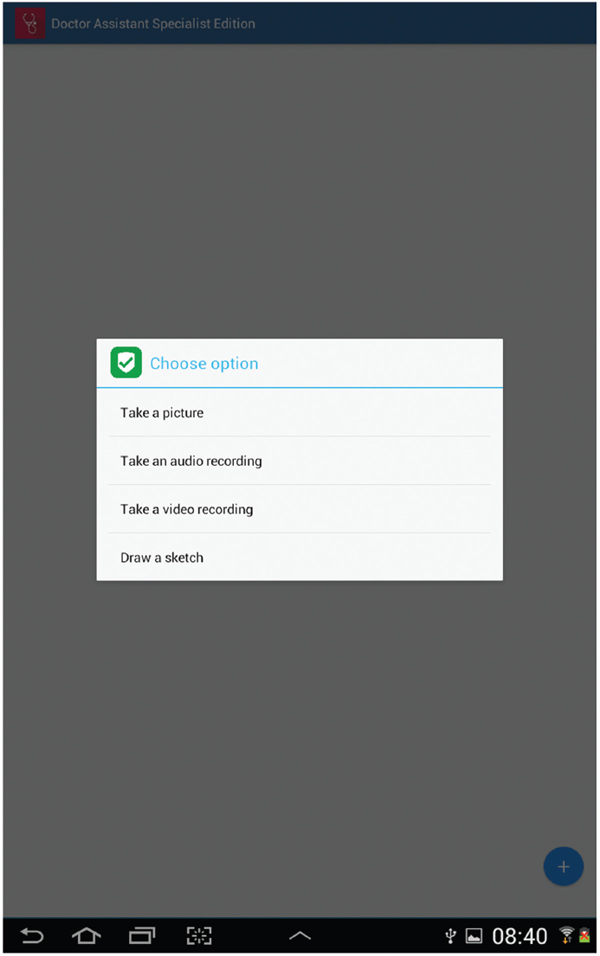
Figure 5 Attachments which can be made are: Picture, Audio recording, Video recording and Sketch.
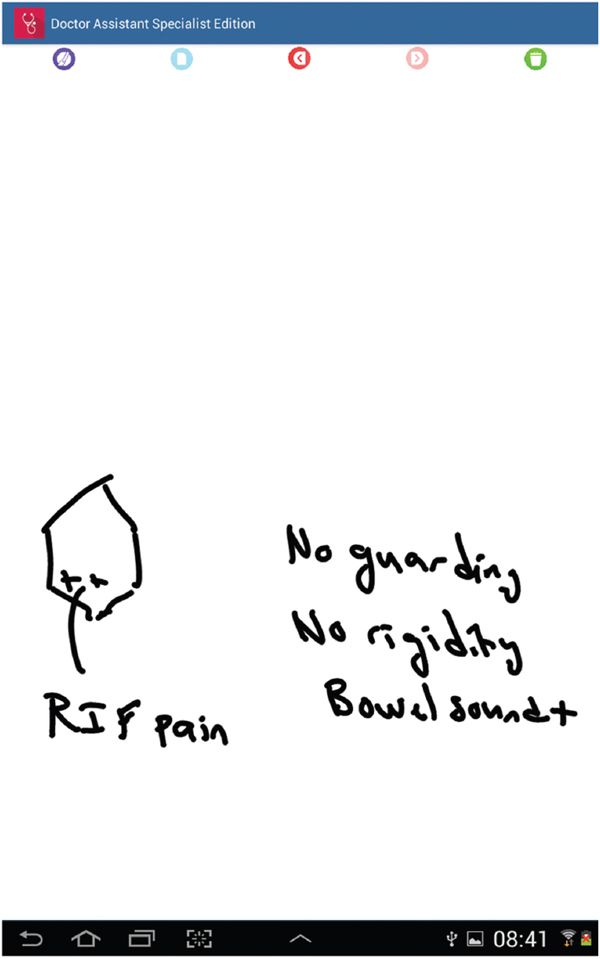
Figure 6 Drawing a sketch is a convenient method for clinicians to document findings.
Mobile technologies are rapidly becoming an essential part of all healthcare services. Mobile devices will be fully integrated into the way that healthcare is designed and delivered. Mobile phones could become the new stethoscopes. Health-related apps have grown in numbers as well as sophistication and impact, with some 100,000 now on the market and many more to come. Whether it is appointment reminders, video demonstrations, social nudging, coaching interactions of any other potential application, mobile is set to become the consumer healthcare communications centerpiece.
In its wider sense, development is about the re-distribution of wealth and growth, ensuring sustainable livelihoods, integrating people who have been left at the margins of society and bridging the digital divide. ICT is an ‘enabler’ and it will dramatically improve the chances of any given country towards meeting its commitments under the Millennium Development Goals (MDG).
5 Doctor Assistant Application
Doctor Assistant application is a free Electronic Medical Record (EMR) application available on Google Play [29]. It has been coded entirely by two practicing Mauritian medical doctors. This user-driven innovation has been downloaded by more than 3000 users worldwide and published in the WHO Compendium of Innovative Health Technologies for Low Resources Settings [30]. The application has been developed through bootstrapping from the two authors’ financial incomes. Doctor Assistant application is supported by 10472 Android devices. The application has 17.48% users from United States, 16.87% from Mauritius, 13.82% from India and 6.10% from Russia. The countries where the application is also used are Egypt, Saudi Arabia, Philippines, South Africa, Bangladesh and Indonesia. The application supports language translation through the Android default settings and the language distribution is 70.01% English, 5.69% Russian, 2.44% Arabic and 1.63% French and 1.22% Italian. The top four application installs by carrier are: 8.33% Cellplus, 3.25% Airtel and 3.25% Verizon Wireless.
In low and middle income countries, the healthcare systems are typically disorganized. Paper-based systems are inefficient and create loss of productivity. Doctor Assistant aims to leverage on the computational power of smart phones to deliver a simple Electronic Medical Record (EMR) for daily clinical usage. The app is designed for Android devices and runs an SQLite Database in background overlaid with a beautiful intuitive graphic user interface (GUI). The application allows unlimited data entry and has a small footprint of 1 MB and barely uses resources from the Android device. The screenshots below demonstrate the core features of Doctor Assistant application.
6 Final Note
Mauritius has the potential to become a platform for health mobile development. The government’s ambition to make Mauritius a Smart Island and ICT as a driver for economic growth may spur more innovative applications in the near future. Mobile application development in healthcare is a niche market of opportunity for Mauritius to emerge as a pioneer in the region and globally.
References
[1] Ure, J., et al., The Development of Data Infrastructures for eHealth: A Socio-Technical Perspective. Journal of the Association for Information Systems, 2009. 10(5): p. 415–429.
[2] Gruber, T., TagOntology – a way to agree on the semantics of tagging data. Retrieved October, 2005. 29: p. 2005.
[3] Alvarez, R.C., The promise of e-Health – a Canadian perspective. Ehealth International, 2002. 1(1): p. 4–4.
[4] Chaudhry, B., et al., Systematic review: impact of health information technology on quality, efficiency, and costs of medical care. Annals of Internal Medicine, 2006. 144(10): p. 742–752.
[5] Kreps, G.L. and L. Neuhauser, New directions in eHealth communication: opportunities and challenges. Patient Education & Counseling, 2010. 78(3): p. 329–336.
[6] Mauritius. Background Notes on Countries of the World: Mauritius, 2009: p. 1.
[7] Ministry of Health and Quality of Life. Health Statitistics Report, Island of Mauritius & Rodrigues. 2013.
[8] ITU - Broadband Commission Strategies for the Promotion of Broadband Services and Infrastructure: A case study on Mauritius. 2012.
[9] Bertelsmann Stiftung, Mauritius Country Report. 2012: http://www.bti-project.org
[10] Southwoord R, The Case for “Open Access” in Africa: Mauritius case study, A.f.P.C. (APC), Editor. 2008: http://www.apc.org/en/pubs/research
[11] Merrill, M. Top 10 factors for successful EHR implementation. 2010 November 2014]; Available from: http://www.healthcareitnews.com/news/top-10-factors-successful-ehr-implementation?single-page=true
[12] Sahin, I., Detailed Review of Rogers’ Diffusion of Innovations Theory and Educational Technology-Related Studies Based on Rogers’ Theory. Online Submission, 2006. 5(2).
[13] Devi, S., Mauritius counts health successes. Lancet, 2008. 371(9624): p. 1567–1568.
[14] Kaplan, B. and K.D. Harris-Salamone, Health IT Success and Failure: Recommendations from Literature and an AMIA Workshop. Journal of the American Medical Informatics Association, 2009. 16(3): p. 291–299.
[15] Wong, M.C., P. Turner, and K.C. Yee, Involving Clinicians in the Development of an Electronic Clinical Handover System – Thinking Systems Not Just Technology. Studies in Health Technology and Informatics, 2008. 136: p. 490–495.
[16] Kessel, K.A., et al., Five-year experience with setup and implementation of an integrated database system for clinical documentation and research. Computer Methods and Programs in Biomedicine, 2014. 114(2): p. 206–217.
[17] De Meyer, F., G. De Moor, and L. Reed-Fourquet, Privacy protection through pseudonymisation in eHealth. Studies in Health Technology & Informatics, 2008. 141: p. 111–118.
[18] Gatzoulis, L. and I. Iakovidis, Wearable and Portable eHealth Systems. IEEE Engineering in Medicine & Biology Magazine, 2007. 26(5): p. 51–56.
[19] Mechael, P., et al., Barriers and gaps affecting mHealth in low and middle income countries: Policy white paper. 2010: Columbia university. Earth institute. Center for global health and economic development (CGHED): with mHealth alliance.
[20] Kaplan, W.A., Can the ubiquitous power of mobile phones be used to improve health outcomes in developing countries. Global Health, 2006. 2(9): p. 1–14.
[21] Franklin, V.L., et al., Patients’ engagement with “Sweet Talk” – a text messaging support system for young people with diabetes. Journal of Medical Internet Research, 2008. 10(2).
[22] Winchester III, W.W., COVER STORY Catalyzing a perfect storm: mobile phone-based HIV-prevention behavioral interventions. interactions, 2009. 16(6): p. 6–12.
[23] Jumreornvong, O., New Weapon In The War Against AIDS: Your Mobile Phone. Intersect: The Stanford Journal of Science, Technology and Society, 2014. 7(1).
[24] O’Donovan, J. and A. Bersin, Controlling Ebola through mHealth strategies. The Lancet. Global health, 2015. 3(1): p. e22.
[25] Societies, C. Taking preventative action to stop the Ebola outbreak in West Africa.
[26] Bengtsson, L., et al., Improved response to disasters and outbreaks by tracking population movements with mobile phone network data: a post-earthquake geospatial study in Haiti. PLoS medicine, 2011. 8(8): p. e1001083.
[27] OpenStreetMap Community Helps With Nepal Earthquake Response Open Health News. 2015 May 2015; Available from: http://www.open healthnews.com/story/2015-05-19/openstreetmap-community-helps-nepal-earthquake-response
[28] Coyle, D., Childs, M.B., The role of mobile phones in disasters and emergencies. 2005, Enlightenment Economics and the GSM Association.
[29] Dr. Bholah Leckraj Amal and Dr. Beharee Kemley. Doctor Assistant. March 2014; Available from: https://play.google.com/store/apps/details? id=com.amakemb.trialrelease.doctorassistanttrial&hl=en
[30] “WHO | Compendium of innovative health technologies for low-resource settings, 2011–2014: Assistive devices, eHealth solutions, medical devices, other technologies, technologies for outbreaks.” Available: http://www.who.int/medical_devices/publications/compendium_iht_low-res-tech/en/
Biographies

L. A. Bholah is a medical doctor with passion in computer programming and electronics. He is a student in the M.Sc. Global eHealth course from University of Edinburgh and also a member of the Commonwealth Youth Health Network. He is author of Doctor Assistant which is a free Electronic Medical Record (EMR) application published in the WHO Compendium of Innovative Health Technologies for Low Resource Settings. He is now the Founder & CEO of Smart Health Ltd which is software and hardware development company specialised in Healthcare.

K. Beharee is a medical doctor who has an intrinsic ability to code software and design hardware for use in healthcare clinical practices. He is passionate about computer science and also code in several programming languages. He is involved in the publication of Doctor Assistant application. He is currently the Chief Technical Officer (CTO) of Smart Health Ltd.
Journal of ICT, Vol. 3, 231–250.
doi: 10.13052/jicts2245-800X.333
© 2016 River Publishers. All rights reserved.