Mobile Health Application for Proactive Self-management: A Case Study of Hypertensive Diabetic Patients in Thailand
Sutussa Sanon and Punnarumol Temdee*
Computer and Communication Engineering for Capacity Building Research Center, School of Applied Digital Technology, Mae Fah Luang University, Chiang Rai, Thailand
E-mail: 6551303013@lamduan.mfu.ac.th; punnarumol@mfu.ac.th
*Corresponding Author
Received 28 June 2024; Accepted 26 December 2024
Abstract
Diabetes and hypertension are prevalent chronic diseases globally. This study was conducted in Thailand and aimed to investigate the impact of a mobile application tailored for promoting self-management of hypertensive diabetic patients. The proposed mobile application provides users with the ability to monitor personal and clinical data and receive personal health recommendations. The recommendations are given according to the health condition trends and personal engagement level of the patient. Health condition detection was used to identify the trends, which can be positive, negative, or neutral progression trends. Personalized recommendations are provided to each patient by investigating personal engagement levels using associate rules. The proposed mobile application was evaluated in terms of effectiveness and user satisfaction for both healthcare professionals and patients in Thailand. The proposed mobile application was considered to be effective at a “moderately high” level (78%) according to 10 healthcare professionals and received an average score of 4.18 out of 5 (“very satisfied”) from 33 patients.
Keywords: Hypertension, diabetes, mobile application, patient modeling, self-management, association rule.
1 Introduction
Non-communicable diseases (NCDs) are prevalent chronic conditions that pose significant health challenges on a global scale. According to the World Health Organization (WHO), NCDs account for approximately 74% of all global deaths, representing a significant public health burden [1]. The rising prevalence of NCDs is largely attributed to unhealthy lifestyle behaviors, encompassing poor dietary choices, physical inactivity, tobacco use, and excessive alcohol consumption. Environmental factors, especially pollution, have been identified as escalating NCDs [2]. Addressing these modifiable risk factors becomes imperative in the prevention and management of NCDs, thereby fostering improved overall population health [3, 4]. Among NCDs, diabetes and hypertension stand out as major concerns. The incidence of type 2 diabetes mellitus (T2DM) has shown a steady increase, affecting a significant proportion of the population, with an estimated 38.4 million people in the United States being affected, accounting for 11.6% of the US population [5]. Notably, 73.6% of individuals with diabetes aged 18 years or older also have hypertension [6].
Diabetes is characterized by a deficiency in insulin production or impaired insulin utilization, leading to elevated blood glucose levels. Diabetes has been strongly associated with an elevated risk of cardiovascular diseases, cerebrovascular accidents, retinopathy, and nephropathy. Diabetes was estimated to cause approximately 1.5 million deaths, with nearly half of these fatalities occurring before the age of 70. It played a significant role in causing around 460,000 deaths associated with kidney disease and approximately 20% of cardiovascular deaths [7]. In Thailand, the prevalence of diabetes in people aged 15 and older is 9.5%, with the highest prevalence in females aged 70–79 years old (24.6%) and males aged 60–69 years old (18.6%). The highest prevalence is in the metropolis area of Bangkok (12.5%), followed by central Thailand (10.6%), northeast Thailand (9.5%), northern Thailand (8.9%), and southern Thailand (6.5%). In terms of diagnosis, 30.6% of people were not diagnosed as having diabetes before, 13.9% were diagnosed but waiting for treatments, 29.3% are on medication but are not achieving good results, and 26.3% have their symptoms under control [8].
Hypertension involves an increase in the force exerted on the walls of the blood vessels. If hypertension fails to be managed, it can lead to severe medical conditions such as renal disease, heart disease, and stroke [9, 10]. The prevalence of hypertension in people aged 15 and older in Thailand is 25.4%, and the group with the highest prevalence is adults aged 80 years and older (76.8%). Central Thailand has the highest prevalence (27.5%), followed by northern Thailand (27.4%), metropolis Bangkok (27.2%), northeastern Thailand (24.3%), and southern Thailand (21.0%). In terms of diagnosis, 57.0% of people were not diagnosed before, 4.1% were already diagnosed but waiting for treatment, 22.0% are on medication but are not achieving good results, and 16.9% have their symptoms under control [10].
Over the years, diabetes and hypertension have contributed significantly to morbidity and mortality rates. This coexistence of conditions is not coincidental but rather a manifestation of the cardiometabolic syndrome, characterized by a cluster of cardiovascular disease (CVD) risk factors encompassing T2DM, hypertension, dyslipidemia, central obesity, and chronic kidney disease [6]. The intricate nature of diabetes and hypertension lies in the severe complications that can profoundly affect individuals’ overall well-being. The rising occurrence of obesity and sedentary behaviors worldwide functions as a major factor driving the growing impact of both diabetes and hypertension, leading to significant healthcare costs, and raising issues in the field of public health. Therefore, it is imperative to effectively manage diabetes and hypertension to mitigate the risk of complications and long-term medical costs.
Recent advancements in technology, including mobile applications, artificial intelligence, and broad internet connectivity, present promising prospects for enhancing long-distance communication and enhancing access to healthcare resources. Similarly, the utilization of mobile apps that aid in managing personal health can bring advantages to individuals dealing with NCDs. These apps allow individuals to efficiently oversee and control their personal health, thereby contributing to an enhanced quality of life. Despite the considerable focus on creating mobile health apps for monitoring the health of NCD patients, there is a lack of emphasis on individuals grappling with both diabetes and hypertension simultaneously.
Despite advancements in medical treatment, many patients fail to protect themselves from complications associated with NCDs because they lack efficient self-management. Self-management is crucial for NCD patients because it will help the patient to manage their own health throughout their health journey. It is believed that self-management is the only effective approach to preserving quality of life and improving health outcomes of NCD patients. At the same time, it involves a dynamic process where individuals actively manage their illness, including tasks such as problem-solving, decision-making, utilizing resources, effective communication with healthcare providers, and acting appropriately [11, 12]. More specifically, self-management involves the preparation and implementation of behavior change procedures that produce desired changes in target behaviors. Self-monitoring is the process of observing and collecting data on your own behavior. Self-evaluation determines how effectively the implemented procedures can change the target behavior. Although self-management is crucial for NCD patients, developing patients’ self-management can be challenging due to the burden of health literacy. However, studies have suggested that mobile health applications are currently a cost-effective and accessible way to promote self-management for patients [13].
Recent advancements in technology, such as affordable health monitoring devices, improved smartphones, and mobile connectivity, have allowed the creation of portable tools to help patients execute self-care plans. Importantly, the portable tools must be efficient and easy to use. This study aimed to create a personalized model specifically to work well with patients who have both hypertension and diabetes. A mobile application is a compelling way to distribute the model in a way that is easy for the patients and provides crucial information in a timely manner, without waiting for a visit to the hospital. Thus, the model was applied to a mobile application and user satisfaction was measured.
2 Literature Review
2.1 Patient Modeling
Patient modeling or patient classification is the process of categorizing patients based on certain characteristics or conditions to facilitate various parts of resource management and treatment planning [14]. This process is essential for ensuring that patients receive the appropriate care and resources based on each patient’s needs. While it does not directly affect the quality of treatment, patient classification can help the organization to operate more efficiently and improve the quality of care in the long term. Currently, patient modeling is extensively utilized for gathering and analyzing data on patient behavior to gain deeper insights into their requirements and preferences, aiding in the decision-making process. It can be used to identify patients who are at risk for not following their treatment plans. The information gained can be used to develop targeted interventions to help patients stay on track with their medication and improve their health conditions [15, 16]. Various methods, such as surveys, questionnaires, in-depth interviews, or direct observations conducted by professionals or tracking devices, can be employed to analyze patients’ characteristics and behaviors [17]. Multiple cases of patient modeling have been noted in the healthcare sector. Patient modeling is frequently utilized to develop a personalized representation or simulation of a patient’s medical characteristics. The model can assist medical professionals in various stages of diagnosis to create treatment plans [18]. Both data-driven and knowledge-based methods are widely adapted for patient modeling. The model can be created using techniques like agent-based methods [19–22] or fuzzy logic-based methods [23–25].
There are various methods that can be used to model hypertension patients including machine learning (ML) based methods [26], such as decision trees, naive Bayes, artificial neural networks, and logistic regression. Furthermore, a modular agent-based model incorporating the pharmacodynamic effects of different antihypertensive medications is used to simulate patient responses to therapies, paving the way for personalized medicine in predicting individual responses to treatment [27]. Overall, these methods showcase promising results in predicting hypertension outcomes and guiding interventions for better patient management. Similarly, ML-based methods are also employed to model diabetic patients and predict outcomes effectively. Various ML algorithms such as logistic regression, random forest, and support vector machines can be utilized for this purpose [28]. These models analyze historical and current data to make informed decisions about patient diagnoses and treatment options, enhancing overall healthcare service quality [29], while achieving high accuracy, indicating their effectiveness in predicting outcomes for diabetic patients.
With the enhancement of computational capabilities in modern computers, ML-based solutions prove advantageous for applications with substantial amounts of collected data. Conversely, a knowledge-based solution is beneficial to those with relatively less data and computational power. Therefore, this study can be considered as an implementation of a knowledge-based system on a mobile health application. More precisely, patient modeling was developed based on the knowledge and expertise of healthcare professionals, incorporating newly proposed factors, like health trends and engagement levels, to provide personalized recommendations.
2.2 Association Rules
Association rules are used to identify items appearing together in datasets. Pairs of items are generated through “if-then” statements, which are easily integrated into mobile applications. Association rules are commonly utilized in marketing analysis to identify frequently purchased item pairs [30]. For example, customers buying ice cream are likely to also purchase chocolate syrup. Various algorithms, such as Apriori algorithm and FP-Growth [30], offer differing speeds, accuracies, and computational capacities, building model improvement. In the healthcare domain, association rules aid in detecting or identifying medical conditions. As demonstrated in [31], association rules can be used to analyze medical records to find common disease pairs. Specifically, [32] applied it to COVID-19 symptom records, while another study [33] utilized it to identify early stages of breast cancer through groups of proteins. From [34], association rules were used to identify correlations between health problems and corresponding treatments, like diabetes and insulin, with reasonable accuracy. Another study [35] generated rules based on sets of binned numeric ranges, such as age, blood glucose, and BMI, to prepare data for the association rule algorithm. Association rules were used in this study to refine the recommendation models.
2.3 Mobile Health (mHealth)
Currently, the existing mobile health (mHealth) applications exhibit a variety of objectives, including symptom monitoring [36], tracking physical activities, providing mental health support, offering general education on specific health issues, and enabling telemedicine [37]. These applications are designed for public use by anyone who can use a smartphone on a regular basis [37]. The advantages of mHealth applications include reduced costs and improved accessibility, thanks to the portability and processing capabilities of modern smartphones, which offer more flexibility compared to earlier feature phones with limited capabilities [38]. The use of mobile health applications has the potential to aid in the management of NCDs, particularly by supporting patients in self-management and encouraging active participation in their own care. This strategy involves setting healthcare goals, ensuring consistent follow-up, and engaging patients in the decision-making process related to treatment protocols and lifestyle modifications that can impact their well-being, with input from data-driven recommendations [2].
There are existing mHealth applications specifically for hypertension and/or diabetes management. One of these applications incorporates extra hardware to provide automated data tracking into the specialized smartphone application, which yielded positive results [39], while others might be relying on manual data entry [40, 41]. Some of these applications offer educational content or motivational messages to users regarding their medical condition, while others provide tailored guidance based on user input data. Additionally, some applications provide a communication channel between the user and a healthcare specialist [42]. Some applications may provide recommendations based on a machine-learning system [43]. Previous research reviews from earlier studies [44, 45] that focused on mobile apps that help diabetes and/or hypertension patients showed that the applications currently found in the smartphone application market are aiming to provide help in self-management without directly involving medical professionals. These applications help patients collect crucial data such as blood glucose and blood pressure levels, alongside activities like exercise, calorie consumption, and medication adherence, while also setting reminders for necessary actions. Educational resources pertaining to the user’s specific medical condition may also be incorporated into certain applications. Generally, individuals utilizing these applications report positive health benefits. Nonetheless, multiple studies from these reviews highlight the potential unreliability or complexity of the application’s usability due to intricate product designs.
The integration of mobile health technologies into healthcare systems still faces various challenges and limitations. These include technical barriers like security and privacy concerns [46], individual barriers such as knowledge and limited literacy [47], and healthcare system barriers like economic and financial factors [48]. Additionally, the adoption of mHealth can be hindered by issues like lack of accessibility and non-standardized medical data across multiple systems [49]. Moreover, the high proliferation of mHealth technologies has raised security and privacy concerns among users, emphasizing the need for well-defined architecture standards to ensure patient data security and privacy [50]. Overcoming these challenges is crucial for the successful integration of mHealth into healthcare systems, requiring a comprehensive approach that addresses technical, individual, and systemic barriers.
3 Methodology
For this study, the research methodology consisted of collecting patient data, creating association rules, applying association rules to the mobile application, and evaluating the mobile application (Figure 1).
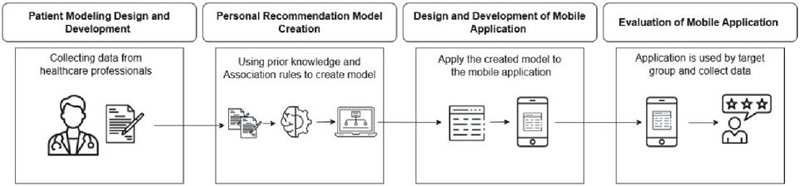
Figure 1 Research methodology steps.
This study covers two experiments that received certificates of approval from the Mae Fah Luang University Ethics Committee on Human Research (protocol number: EC 23065-13 on September 21, 2023 and EC 24105-13 on October 4, 2024). The detail of each process is discussed here.
3.1 Patient Modeling Design and Development
For this study, patient modeling incorporated the engagement level and condition progression trend as shown in Figure 2.
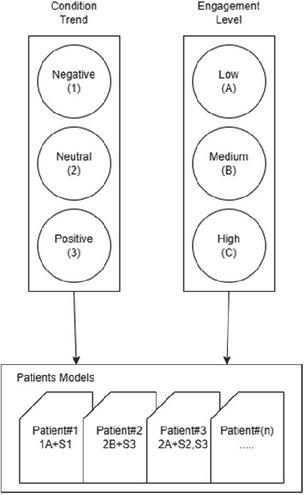
Figure 2 Proposed patient modeling.
The engagement levels and condition trends were obtained from the perspective of healthcare professionals, who were responsible for hypertensive diabetes patients. More details of each process are described in this section.
3.1.1 Engagement levels
The engagement levels were derived from an analysis of healthcare experts’ perspectives. The interview was conducted with 10 healthcare experts in the appropriate field to extract their experience on classifying and treatment of patients. The survey questionnaires were also completed by them to extract important features used for patient modeling and recommendations. Questions in both the interviews and survey questionnaire were evaluated by three experts in total, two in the healthcare domain and one in the mobile application development domain. Questions for the healthcare experts focused on the patient care process, planning the appropriate treatments, and what to do if the patient is not adhering to the treatment. These questions were open-ended questions to allow the condensed version of the care plan that was integrated into the recommendation. From the interview and survey questions, the patient’s level of engagement, which is how strictly the patient followed the given recommendation, was determined. This study categorized patients into three groups according to their engagement level: low, medium, and high. The definition of each level is shown in Table 1.
Table 1 Engagement level and explanation
| No. | Engagement Levels | Explanation |
| 1 | Low | Patient compliance: 40%. For example, the patient did not take half or more of their prescribed medicine, did not follow the recommended diet for more than 2 days per week, did not perform exercise for more than 2 days per week. |
| 2 | Medium | Patient compliance: 40–70%. For example, the patient did not take all their medication for less than 2 days per week, followed the diet for less than 2/3 of the week, performed exercise for less than 4 days per week. |
| 3 | High | Patient compliance: 70%. For example, the patient takes medicine to the prescribed dosage every day, eats the recommended diet for more than 1/2 of the week, performs 30 minutes of exercise 5 days a week. |
From Table 1, the engagement level operates on the adherence of the patient to the recommendation given by the healthcare expert. Majority opinions were used to determine the exact thresholds of all activity frequencies.
3.1.2 Condition progression trend
In this study, a model of the condition progression trend was employed to detect the direction of change in a patient’s symptoms based on health metrics such as blood pressure, body weight, blood sugar level, and other metrics using standardized ranges. This model categorizes the progression trends into three categories to cover the possibilities of changes according to the previous work [51]. The specific items defining these categories can be found in Table 2.
Table 2 Condition progression trends and explanation
| No. | Condition Progression Trends | Explanation |
| 1 | Positive Condition Progression Trend | The patient has progressive health status, moving towards the known good range of the metric, such as lowering body weight towards the “healthy” range from the “overweight” range. |
| 2 | Negative Condition Progression Trend | The patient has regressive health status, moving away from the known good range of the metric, such as gaining body weight, moving away from the “overweight” range into the “obese” range. |
| 3 | Neutral Condition Progression Trend | The patient has little to no change of health status within the margin, such as maintaining the body weight within the “healthy” range, keeping the average weight without significantly moving towards other ranges. |
The positive condition progression trend indicates improvement, as clinical values shift closer to those of asymptomatic or normal individuals. The negative condition progression trend reflects deterioration, with values moving further from normal ranges. For individuals in a stable condition, the neutral progression trend tracks symptom progression. These metrics help guide patients in seeking further healthcare recommendations.
3.1.3 Patient modeling
The patient modeling, composed of the condition progression trend and engagement level, was used to create sets of associated recommendations for patients. For this study, the types of patient modeling are shown in Table 3.
Table 3 Types of patient modeling
| No. | Tag | Explanation |
| 1 | 1A | Patient has negative trend and low engagement |
| 2 | 1B | Patient has negative trend and medium engagement |
| 3 | 1C | Patient has negative trend and high engagement |
| 4 | 2A | Patient has neutral trend and low engagement |
| 5 | 2B | Patient has neutral trend and medium engagement |
| 6 | 2C | Patient has neutral trend and high engagement |
| 7 | 3A | Patient has positive trend and low engagement |
| 8 | 3B | Patient has positive trend and medium engagement |
| 9 | 3C | Patient has positive trend and high engagement |
From Table 3, it can be seen that different patient profiles could be constructed based on their engagement levels and condition trend. Different patients’ profiles should obtain different recommendations. For example, patient 1A has a negative progression trend compared to the last diagnosis time and a low engagement. Therefore, patients 1A and 1C should obtain different recommendations because they have different engagement levels. The recommendation construction is described in the next section.
3.2 Personal Recommendation Model
Using the patient engagement level (low, medium, and high) and condition progression trend (positive, negative, and neutral), individual recommendations were constructed. A conceptual diagram of recommendation construction is shown in Figure 3.
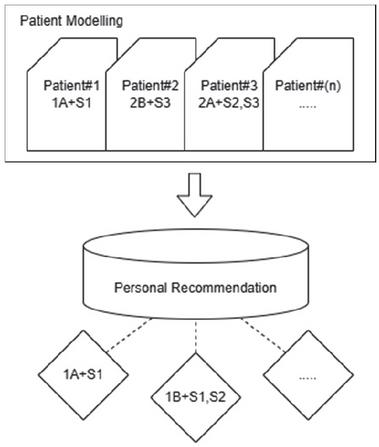
Figure 3 Personalized recommendation construction.
The general recommendations that the healthcare professional normally give to the all patients were critically matched to the individual patients based on their different profiles using association rules, according to the perspective of the healthcare professional. Table 4 shows general recommendations normally given to all patients.
Table 4 Set of general recommendations
| No. | Recommendation | Explanation |
| 1 | Advise | Expert gives general advice to patient |
| 2 | Educate | Expert gives in-depth education to patient |
| 3 | Encourage | Expert gives encouragement to patient |
| 4 | Solo-session | Expert arranges private talk with patient along with caretaker |
| 5 | Group-session | Expert arranges group talk with multiple patients with a team of professionals |
| 6 | Home-check | Expert sets a home visit session appointment |
| 7 | Monitor | Expert sets a monitoring program for patient |
| 8 | Reconsider | Expert reconsiders the current treatment plan |
| 9 | Follow-up | Expert sets follow-up appointment |
The general recommendations for managing hypertensive diabetic patients should factor in the patient’s food consumption, medication, and exercise. External aspects like family influence and socioeconomic factors are also important; however, they were not considered in this study. Patients generally follow the provided dietary guidelines and advice, but they may become less strict as time passes. For example, families can become intentionally less strict to make the patient happy or patients can completely neglect the plan due to a lack of caretaker support.
Positive encouragement is recommended for patients who are successfully following the treatment plan, whereas those who are unwilling to follow the plan may need extra consideration and proactive support by providing societal encouragement and additional education to highlight the potential consequences. Additionally, group sessions are an effective way to provide support from both the healthcare experts and the members of the group, after which individual consulting sessions or home visits may be provided. Care plans should also fit with the patient’s condition. To create personal recommendations, association rules were used to model the appropriate recommendation based on different patient profiles from the healthcare professionals’ perspectives.
3.2.1 Personal recommendation construction
Association rules are a technique used to uncover interesting relationships or patterns between variables in large datasets. These rules are particularly useful for identifying frequent patterns, correlations, or associations among sets of items. More specifically, they are a powerful tool for extracting actionable insights from large datasets, helping businesses make data-driven decisions. Three measurements from association rule mining are used to construct the rules for employment in mobile applications: support, confidence, and lift.
The support value refers to how often a certain set of items appears in the dataset. The higher the number of supports, the more common they appear. It can be calculated by Equation (1).
| (1) |
where x is the antecedent item – an individual item that appears in the record, y is the consequence item – a different individual item that appears later in the record, s is the support value of x appears together with y, r({x},{y}) is the number of records where x and y are in the same record, and t denotes the total number of records in the database.
The confidence value is how likely it is if the condition has x and will also have y. A higher number indicates that the first item is more likely to cause the second item to appear in the same record. It can be calculated by Equation (2).
| (2) |
where x is the antecedent item – an individual item that appears in the record, y is the consequence item – a different individual item that appears later in the record, c is the confidence value of x appears together with y, r({x},{y}) is the number of records where x and y are in the same record, and r{x} is the number of records in which only x was recorded in the database.
The lift value is the ratio of when the condition is y when x occurs first. A value greater than 1 means that x and y have a positive relationship, as in, x will cause y to occur more. A value of less than 1 means that x and y have a negative relationship, as in, x causing y to occur less. It can be calculated by Equation (3).
| (3) |
where x is the antecedent item – an individual item that appears in the record, y is the consequence item – a different individual item that appears later in the record, l is the lift value of x appears together with y, c({x}{y}) is the confidence value where x appears together with y, and s{x} is the support value in which only y is in the record.
These values are crucial in the calculation of the association rules. Certain rules may have a lower occurrence and thus could be pruned if their support and confidence metrics fall below a certain threshold.
Data were collected from the eight interviewed healthcare experts and reviewed by two other healthcare experts, for a total of 10 experts. Therefore, 72 records were used to calculate the initial association rules. The resulting rules are presented in Table 5.
Table 5 Sample of key metrics of association rules
| Profile: Model | Recommendation | Support | Confidence | Lift |
| 1A: Negative Condition + Low Engagement | Educate | 0.097 | 0.875 | 2.520 |
| 1B: Negative Condition + Medium Engagement | Encourage | 0.069 | 0.625 | 1.000 |
| 1C: Negative Condition + High Engagement | Reconsider | 0.111 | 1.000 | 2.880 |
| 2A: Neutral Condition + Low Engagement | Educate | 0.097 | 0.875 | 2.520 |
| 2B: Neutral Condition + Medium Engagement | Encourage | 0.097 | 0.875 | 1.400 |
| 2C: Neutral Condition + High Engagement | Encourage | 0.111 | 1.000 | 1.600 |
| 3A: Positive Condition + Low Engagement | Educate | 0.097 | 0.875 | 2.520 |
| 3B: Positive Condition + Medium Engagement | Encourage | 0.069 | 0.625 | 1.000 |
| 3C: Positive Condition + High Engagement | Encourage | 0.111 | 1.000 | 1.600 |
To demonstrate how to calculate the metric values, the first association rule “Negative Condition + Low Engagement Educate” was selected for demonstration.
From the 72 records in the dataset, there were 7 instances of 1A+S2 (Negative Condition and Low Engagement + Educate), 8 instances of 1A and 25 instances of S2. This means the support value of the antecedent was (7/72) or 0.097. The confidence value of the rule was calculated using the support value of the antecedent divided by the support value of the consequent item, in this case, the confidence value was (7/72) / (8/72) 0.875. The lift value was calculated using the confidence value divided by the confidence of the consequent item; therefore, the lift value of the rule “Negative Condition + Low Engagement Educate” was (7/8) / (25/72) 2.52.
For this study, association rules were used in conjunction with patient modeling to provide customized recommendations to the individual patients. Table 6 shows examples of constructed personal recommendations.
Table 6 Sample of personal recommendation rules
| No. | Recorded data |
| 1 | 3B, follow-up |
| 2 | 2B, follow-up, reconsider, encourage |
| 3 | 1B, home-check, encourage, reconsider |
| 4 | 3A, follow-up, educate |
| 5 | 2A, follow-up, educate |
| 6 | 1A, home-check, educate |
| 7 | 3C, encourage |
| 8 | 2C, encourage, reconsider |
| 9 | 1C, reconsider, educate |
| 10 | 3B, encourage |
If a patient with a low engagement level gains weight, which is marked as a negative condition trend (1A), the personal recommendation will be assigning a home check and educating the patient more about their conditions. As this rule was created after the association mining found this pattern in the experts’ interviews, this set of actions is sent to the application. After the rules were created, they were compared with the original rules provided by the experts by matching the consequence between the original and the generated rule for each antecedent rule. Then, the matched percentage was evaluated. A higher percentage means that the generated rules match more from the possible answers from the experts’ opinions. Considering that one antecedent set may have multiple answers for the consequences, the percentage was based on the amount of all answers that match within the answer list. For example, the Negative Condition + Low Engagement antecedent had the following answers from the experts: 1 Educate, 1 Reconsider and 3 Encourage, if the generated rule was ‘Educate’, the matched percentage was 20% (1/5 answers). If the generated rule was ‘Encourage’, the matched percentage was 60% (3/5 answers).
3.3 Design and Development of Mobile Application
3.3.1 Application design phase
For this process, the design stage involved the systematic development of a structured framework for creating a software application. Specifically tailored to diabetes and hypertension management, this stage focused on the intricate design and conceptualization of a user-oriented mobile application. This design process has the potential to significantly enhance the efficacy of chronic disease management for its intended user base. Figure 4 presents the use case of the care management actors, and Table 5 describes this use case in detail.
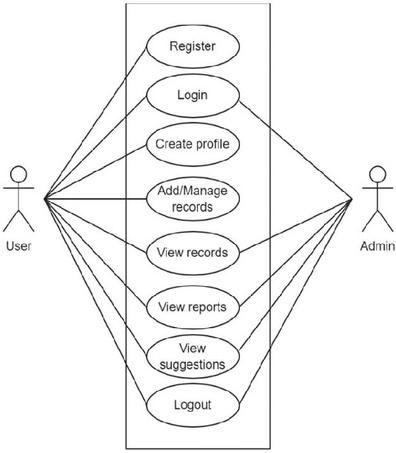
Figure 4 Use case for patient and administrator.
| Actor | Use Case | Use Case Description |
| Patient | Registration | Patient must register a profile before using the application |
| Login | Patient has been authenticated to use the application | |
| Records | Patient can log their activities and bodily data | |
| Report | Patient can access and review their history and reports | |
| Suggestions | Patient can view the suggestions made by the prediction system | |
| Logout | Patient can remove their account from the application | |
| Admin | Login | Administrator must login before doing any action on the application |
| Records | Administrator can edit information within the application. | |
| Report | Administrator can access and view reports in the system | |
| Logout | Administrator can exit the application |
There are two types of users in the system. The patients, otherwise known as normal users, and the administrators. Users will be able to register an account and create their profile, and they can add and manage records of their health data as well as view previous records and the reports and recommendations created by the personalized model. Lastly, the user can log out of their account if they wish to move to a different device. The administrator can log into the system to retrieve all records submitted by the users for analytics, plus the generated reports and suggestions of each user. The administrator can also log out when they have finished their data retrieval.
3.3.2 Mobile application development phase
For this process, the objective was to develop a mobile application capable of receiving user information, processing data, and providing suitable advice, specifically targeting the elderly user group. Therefore, it was imperative to design an easy-to-use interface. The proposed mobile application is running on the Android mobile operating system for easy installation. Figure 5 shows a diagram of the mobile application development process.
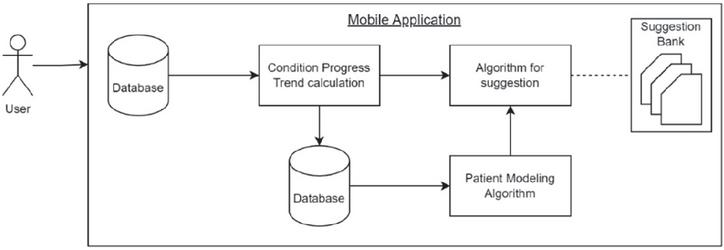
Figure 5 Mobile application development diagram.
The application connects to a private server that stores user data. User input is received and stored within the server, allowing for easy data retrieval and processing. The key functionalities of the mobile application encompass personal information management, disease information tracking, consumption tracking, activity monitoring, and provision of health care advice. Data storage was done using a private web server with database storage and calculation service on the same server for quick responses in data processing.
3.4 Evaluation of Mobile Application
An evaluation of the developed mobile application was conducted to study user satisfaction. A survey questionnaire was used in conjunction with the five-item Likert Scale to measure user satisfaction. The survey questions for usability testing and the obtained results are presented in the next section. The average number of the answer value was selected to represent the general feelings of the user based on a scale of 1 to 5. The number ranges and their explanations can be found in Table 8.
Table 8 Likert scale average score explanation
| Averaged Value | Meaning |
| 4.50 to 5.00 | Strongly agree / Very satisfied |
| 3.50 to 4.49 | Agree / Somewhat satisfied |
| 2.50 to 3.49 | Neither agree nor disagree / Neither satisfied nor dissatisfied |
| 1.50 to 2.49 | Disagree / Somewhat dissatisfied |
| 1.00 to 1.49 | Strongly disagree / Very dissatisfied |
The satisfaction survey was conducted on the target group of caretakers who are on duty helping hypertensive diabetic patients. Thirty-three participants completed the survey after using the application for 2 weeks. Each answer was interpreted by reading the average value of that question and comparing it with the meanings to combine into a single statement. For example, a score of 4.59 on the question means the users generally strongly agree with that question.
4 Results and Discussion
4.1 Effectiveness of Personal Recommendation Model
The constructed rules were compared with the recommendations of 10 healthcare experts. The effectiveness of the constructed rules is presented in terms of the matched percentage between constructed rules (Table 9).
Table 9 Matched percentage of constructed rules
| No. | Antecedent Condition Trend | Matched Percentage |
| 1 | Negative Condition + Low Engagement | 28.00% |
| 2 | Negative Condition + Medium Engagement | 15.00% |
| 3 | Negative Condition + High Engagement | 5.88% |
| 4 | Neutral Condition + Low Engagement | 8.00% |
| 5 | Neutral Condition + Medium Engagement | 38.89% |
| 6 | Neutral Condition + High Engagement | 41.67% |
| 7 | Positive Condition + Low Engagement | 5.00% |
| 8 | Positive Condition + Medium Engagement | 50.00% |
| 9 | Positive Condition + High Engagement | 72.73% |
The generated rules were compared to the original data provided by healthcare experts and the matched percentage was calculated. For example, if there were 10 answers in the category and the generated rules matched with 7 answers in the category, the matched percentage was 70%. A higher matched percentage in a category indicates that the actions (educate, follow-up, etc.) were matched with the answers given by the experts. A lower percentage indicates that the generated rules differed from the original data.
The findings indicate that the association rules worked well to find the appropriate rules even with the limited amount of data that was collected from the professionals. Although the confidence of the rules was limited, the rules generated were effective enough to gain high matched percentages. Some of the generated rules showed that encouragement towards patients is important. Giving positive reinforcement might help improve the mentality of the patients to keep on improving their health. In addition, straightforward education of the negative consequences is an effective way to encourage patients to take care of their health.
The wide range of the matched percentages could be attributed to the low sample size of the original data and the lack of agreement between answers in a category after the rule generation. This issue may be improved by collecting more data on treatment plans from multiple healthcare providers and experts in similar fields.
4.2 Mobile Application Interfaces
The development of the mobile application focused on the main functionality of collecting data while also being easy to use and having a simple design of menu navigation that is common to other mobile applications in the market to reduce the time needed to learn how to use the application. Sample images of the user interface with translated labels are shown in Figure 6.

Figure 6 Examples of mobile application interfaces.
To use the application, the user must register an account and enter basic information such as birth date, body weight in kilograms, height in centimeters, type of chronic disease, and gender. The full name is only displayed within the application. The email address and password are to authenticate the user and allow access to the information.
The home page displays the metrics from previous data collection, which are presented in easy-to-read graphics. The user can tap on a display card to view that metric. The data page is where the user enters their data. Depending on the type of data that the user has selected, the form will change to accept that specific type of data. For example, If the user selects to enter their BMI, only weight and height forms will be presented to the user. The stats page is a summary of the changes using the Patient Recommendation model to display the current health metrics and recent changes in the direction of each metric. The recommendation text in the card can change based on the trend and conditions and gives out the action that the user should be taking to improve their health. More pages used for presenting personal information and recommendations are shown in Figure 7.
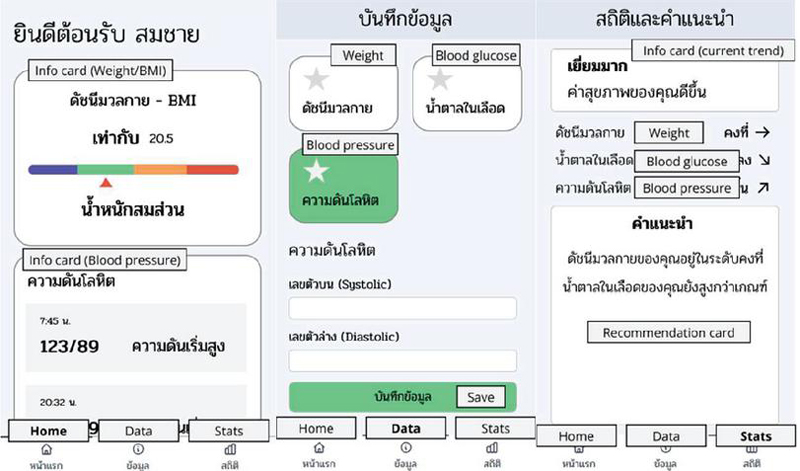
Figure 7 Personal information and recommendation pages.
When the application detects a significant change in the condition of a patient, whether they have diabetes, hypertension, or both, the application will send a recommendation to the user on certain topics such as exercise or diet changes. The provided recommendations from the application should be treated by the user as a basic suggestion and not medical advice from a professional. Experts may use the information from the mobile application to prescribe appropriate treatments after consideration. The user is encouraged to use the application daily to submit data at the same time every day to ensure the consistency of the data, as there can be variances due to lifestyle and activity if collected at different times. The application provides a simple reminder notification at the user-selected time to remind them to use the application.
4.3 Satisfaction with the Mobile Application
4.3.1 Patient satisfaction
A list of questions and response scores for investigating the satisfaction from using the application are shown in Table 10.
Table 10 Survey questions and responses
| Questions | AVG | SD |
| Recommendation is easy to understand | 4.18 | 6.43 |
| Recommendation is appropriately personalized | 3.94 | 5.77 |
| Recommendation is complete with information | 3.91 | 7.16 |
| Recommendation can be used daily | 4.21 | 6.62 |
| Function is useful for daily lifestyle improvements | 4.27 | 7.57 |
| Function has variety in recommendations | 4.00 | 5.59 |
| Application is easy to understand | 4.15 | 6.31 |
| Application is well-designed | 4.30 | 7.30 |
| Application feels fast and responsive | 4.30 | 7.23 |
| Application feels secure in storing information | 4.39 | 7.96 |
| Basic functions are easy to use | 4.27 | 7.02 |
| Texts in application are easy to read | 4.21 | 6.91 |
| Color usages are clear to read | 4.33 | 7.64 |
| Overall satisfaction with using application | 4.09 | 6.31 |
| Abbreviations: AVG Average Likert Scale score of the questions, SD Standard Deviation of the Likert Scale. | ||
The result of the survey shows a high level of satisfaction among the users. The average score was within the satisfactory range, expressing users’ satisfaction with the application. Patients gave positive comments about how the application was easy to use and felt secure for storing personal information. There were some negative comments about the recommendation system, indicating that it showed incorrect predictions due to insufficient personal data and that the instructions were unclear in some functions.
There are concerns about the accessibility of mobile devices to people outside the research program. For some groups of people, smartphones are expensive in terms of the upfront cost and maintenance of services that are needed such as cell services and electricity. Older people might have difficulty operating the device due to a lack of finger dexterity, which means that smartphone devices might not be the best fit for this group of people. The application was designed to target middle-aged people who may have the chronic disease themselves or might be caring for elders. Thus, it requires a high level of digital literacy, the ability to read, and knowledge of how to use smartphones safely.
Potential plans to improve the application for future development include the following: (1) modification to accept a wider range of personal health data, such as approximate sleep time and exercise, as a way to determine the activity level of the user and help with the prediction model, (2) modification to add direct communication from a healthcare service to the user as a way to provide in-depth guidance using the collected data, and (3) localization and translation into other languages to support a wider user base.
5 Conclusion
This study aimed to propose a mobile application to promote proactive self-management for hypertensive diabetes patients in Thailand. More specifically, this study proposed patient modeling using patient engagement levels, which were derived from the perspectives of healthcare professionals, and condition progressive trends. The recommendations were constructed using association rules customizing general recommendations into personal recommendations for the patients individually. For this study, nine rules were constructed, and they were evaluated in terms of effectiveness by comparing them to the opinions of 10 healthcare experts. The accuracy of the prediction model ranged from 5% to 72.73%. In addition, the mobile application was assessed in terms of satisfaction by 33 patients. The developed mobile application obtained an average Likert score of 4.18 out of 5 from the patients, indicating a moderate level of satisfaction. Future research should focus on long-term impact evaluation and continuous improvement based on user feedback and emerging technologies.
Acknowledgments
This study is part of a research project entitled “Proactive Self-Management Mobile Application for Chronic Patients: A Case Study of Hypertensive Diabetic Patients in Chiang Rai (2nd year)”, and funded by the Basic Research Fund 2023, Thailand Science Research and Innovation (TSRI).
References
[1] World Health Organization, ‘Noncommunicable diseases’, World Health Organization, Sep. 16, 2023. https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases.
[2] I. H. de Boer et al., ‘Diabetes and hypertension: A position statement by the American Diabetes Association’, Diabetes Care, vol. 40, no. 9, pp. 1273–1284, Aug. 2017, https://doi.org/10.2337/dci17-0026.
[3] G. Caprara, ‘Mediterranean-type dietary pattern and physical activity: the winning combination to counteract the rising burden of non-communicable diseases (NCDs)’, Nutrients, vol. 13, no. 2, p. 429, Jan. 2021, https://doi.org/10.3390/nu13020429.
[4] NCD Alliance, ‘NCDs |NCD Alliance’, ncdalliance.org, 2019. https://ncdalliance.org/why-ncds/NCDs.
[5] Centers for Disease Control and Prevention, ‘National diabetes statistics report’, CDC, Nov. 29, 2023. https://www.cdc.gov/diabetes/data/statistics-report/index.html.
[6] S. Naha, M. J. Gardner, D. Khangura, L. R. Kurukulasuriya, J. R. Sowers, ‘Hypertension in diabetes’, in Endotext, South Dartmouth (MA): MDText.com, Inc., Aug. 2021. https://www.ncbi.nlm.nih.gov/books/NBK279027/.
[7] World Health Organization, ‘Diabetes’, World Health Organization, Apr. 05, 2023. https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed Jul. 05, 2023).
[8] W. Aekplakorn, ‘The Thai National Health Examination Survey VI (NHES VI)’, 2021. https://online.fliphtml5.com/bcbgj/znee/\#p=202 (accessed Mar. 03, 2024).
[9] Z. Wang, T. Yang, H. Fu, ‘Prevalence of diabetes and hypertension and their interaction effects on cardio-cerebrovascular diseases: a cross-sectional study’, BMC Public Health, vol. 21, no. 1, Jun. 2021, https://doi.org/10.1186/s12889-021-11122-y.
[10] World Health Organization, ‘Hypertension’, World Health Organization, Mar. 16, 2023. https://www.who.int/news-room/fact-sheets/detail/hypertension (accessed Jul. 05, 2023).
[11] M. A. Powers et al., ‘Diabetes self-management education and support in type 2 diabetes: A joint position statement of the American Diabetes Association, the American Association of Diabetes Educators, and the Academy of Nutrition and Dietetics’, Diabetes Care, vol. 38, no. 7, pp. 1372–1382, Jun. 2015, https://doi.org/10.2337/dc15-0730.
[12] J. M. Cramm, A. P. Nieboer, ‘Self-management abilities, physical health and depressive symptoms among patients with cardiovascular diseases, chronic obstructive pulmonary disease, and diabetes’, Patient Education and Counseling, vol. 87, no. 3, pp. 411–415, Jun. 2012, https://doi.org/10.1016/j.pec.2011.12.006.
[13] R. Li, N. Liang, F. Bu, T. Hesketh, ‘The effectiveness of self-management of hypertension in adults using mobile health: systematic review and meta-analysis’, JMIR mHealth and uHealth, vol. 8, no. 3, p. e17776, Mar. 2020, https://doi.org/10.2196/17776.
[14] L. Fagerstrom, K. Eriksson, I. B. Engberg, ‘The patient’s perceived caring needs: Measuring the unmeasurable’, International Journal of Nursing Practice, vol. 5, no. 4, pp. 199–208, Dec. 1999, https://doi.org/10.1046/j.1440-172x.1999.00172.x.
[15] A. M. Chudyk et al., ‘Models and frameworks of patient engagement in health services research: a scoping review protocol’, Research Involvement and Engagement, vol. 4, no. 1, Sep. 2018, https://doi.org/10.1186/s40900-018-0111-5.
[16] F. B. Hailu, A. Moen, P. Hjortdahl, ‘Diabetes self-management education (DSME) – effect on knowledge, self-care behavior, and self-efficacy among type 2 diabetes patients in Ethiopia: A controlled clinical trial’, Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy, vol. 12, no. 1, pp. 2489–2499, Nov. 2019, https://doi.org/10.2147/dmso.s223123.
[17] S. Gupta, J. Agarwal, ‘Machine learning approaches for student performance prediction’, in 2022 10th International Conference on Reliability, Infocom Technologies and Optimization (Trends and Future Directions) (ICRITO), pp. 1–6. https://doi.org/10.1109/ICRITO56286.2022.9964821.
[18] S. G. Elkhuizen, Jan, M. Mahdavi, van, ‘Modeling patient journeys for demand segments in chronic care, with an illustration to type 2 diabetes’, Frontiers in Public Health, vol. 8, 2020, https://www.frontiersin.org/journals/publichealth/articles/10.3389/fpubh.2020.00428.
[19] T. Dudkina, I. Meniailov, K. Bazilevych, S. Krivtsov, A. Tkachenko, ‘Classification and prediction of diabetes disease using decision tree method’, in IT&AS, 2021, pp. 163–172.
[20] F. Mercaldo, V. Nardone, A. Santone, ‘Diabetes mellitus affected patients classification and diagnosis through machine learning techniques’, Procedia computer science, vol. 112, pp. 2519–2528, 2017.
[21] S. G. Nejad, R. Paranjape, ‘An agent model of a diabetic patient’, in 2007 Canadian Conference on Electrical and Computer Engineering, pp. 214–218. https://doi.org/10.1109/CCECE.2007.59.
[22] L. A. AlKaabi, L. S. Ahmed, M. F. Al Attiyah, M. E. Abdel-Rahman, ‘Predicting hypertension using machine learning: Findings from Qatar Biobank Study’, PLOS ONE, vol. 15, no. 10, p. e0240370, Oct. 2020, https://doi.org/10.1371/journal.pone.0240370.
[23] N. Rachata, W. Rueangsirarak, C. Kamyod, P. Temdee, ‘Fuzzy near compactness based personalized recommendation for preventing patients with type 2 diabetes mellitus and hypertension from cardiovascular complication’, Wireless Personal Communications, vol. 115, no. 4, pp. 3073–3097, Jun. 2020, https://doi.org/10.1007/s11277-020-07532-7.
[24] N. Rachata, P. Temdee, ‘Personalized recommendation for preventing patients with type 2 diabetes mellitus and hypertension from cardiovascular complication’, in 2018 Global Wireless Summit (GWS), Nov. 2018. https://doi.org/10.1109/gws.2018.8686590.
[25] N. Rachata, P. Temdee, W. Rueangsirarak, C. Kamyod, ‘Fuzzy based risk predictive model for cardiovascular complication of patient with type 2 diabetes mellitus and hypertension’, ECTI Transactions on Computer and Information Technology (ECTI-CIT), vol. 13, no. 1, pp. 49–58, Jun. 2019, https://doi.org/10.37936/ecti-cit.2019131.132114.
[26] E. Dritsas, S. Alexiou, K. Moustakas, ‘Efficient datadriven machine learning models for hypertension risk prediction’, in 2022 International Conference on INnovations in Intelligent SysTems and Applications (INISTA), pp. 1–6. https://doi.org/10.1109/INISTA55318.2022.9894186.
[27] W. Ji, Y. Zhang, Y. Cheng, Y. Wang, Y. Zhou, ‘Development and validation of prediction models for hypertension risks: A cross-sectional study based on 4,287,407 participants’, Frontiers in Cardiovascular Medicine, vol. 9, Sep. 2022, https://doi.org/10.3389/fcvm.2022.928948.
[28] G. Singh, Mamta, J. Singh, Muskan Gahlawat, ‘Prominent prediction model for chronic diabetes disease using machine learning’, 2022 6th International Conference on Electronics, Communication and Aerospace Technology, Dec. 2022, https://doi.org/10.1109/iceca55336.2022.10009399.
[29] J. Mythili, T Surendhar, P. Suryaprakash, K. Suresh Kumar, ‘Machine learning techniques for diabetes prediction: A comparative analysis’, Jun. 2023, https://doi.org/10.1109/icscss57650.2023.10169658.
[30] T. A. Kumbhare, S. V. Chobe, ‘An overview of association rule mining algorithms’, International Journal of Computer Science and Information Technologies, vol. 5, no. 1, pp. 927–930, 2014,
[31] M. Tandan, Y. Acharya, S. Pokharel, M. Timilsina, ‘Discovering symptom patterns of COVID19 patients using association rule mining’, Computers in Biology and Medicine, vol. 131, p. 104249, 2021, https://doi.org/10.1016/j.compbiomed.2021.104249.
[32] L. K. S, G. Vadivu, ‘A novel approach for disease comorbidity prediction using weighted association rule mining’, Journal of Ambient Intelligence and Humanized Computing, 2019, https://doi.org/10.1007/s12652019012171.
[33] N. Domadiya, U. P. Rao, ‘Privacy preserving association rule mining on distributed healthcare data: COVID-19 and breast cancer case study’, SN Computer Science, vol. 2, no. 6, Aug. 2021, https://doi.org/10.1007/s42979-021-00801-7.
[34] A. Wright, E. S. Chen, F. L. Maloney, ‘An automated technique for identifying associations between medications, laboratory results and problems’, Journal of Biomedical Informatics, vol. 43, no. 6, pp. 891–901, Dec. 2010, https://doi.org/10.1016/j.jbi.2010.09.009.
[35] B. M. Patil, R. C. Joshi, D. Toshniwal, ‘Association rule for classification of type2 diabetic patients’, in 2010 Second International Conference on Machine Learning and Computing, pp. 330–334. https://doi.org/10.1109/ICMLC.2010.67.
[36] K. Tsang, H. Pinnock, A. Wilson, S. Shah, ‘Application of machine learning algorithms for asthma management with mHealth: A clinical review’, Journal of Asthma and Allergy, vol. 15, pp. 855–873, Jun. 2022, https://doi.org/10.2147/JAA.S285742.
[37] O. Haggag, J. Grundy, M. Abdelrazek, S. Haggag, ‘A large scale analysis of mHealth app user reviews’, Empirical Software Engineering, vol. 27, no. 7, Oct. 2022, https://doi.org/10.1007/s10664-022-10222-6.
[38] J. McCool, R. Dobson, R. Whittaker, C. Paton, ‘Mobile health (mHealth) in low- and middle-income countries’, Annual Review of Public Health, vol. 43, no. 1, Oct. 2021, https://doi.org/10.1146/annurev-publhealth-052620-093850.
[39] N. Sakane et al., ‘The effect of a mHealth app (KENPO-app) for specific health guidance on weight changes in adults with obesity and hypertension: Pilot randomized controlled trial’, JMIR mHealth uHealth, vol. 11, p. e43236, 2023, https://doi.org/10.2196/43236.
[40] S. W. Oh, K.-K. Kim, S. S. Kim, S. K. Park, S. Park, ‘Effect of an integrative mobile health intervention in patients with hypertension and diabetes: crossover study’, JMIR mHealth and uHealth, vol. 10, no. 1, p. e27192, Jan. 2022, https://doi.org/10.2196/27192.
[41] J. Paluyo, A. Stake, R. Bryson, “Padayon’: a new digital health model for diabetes and hypertension in rural Philippines’, BMJ Innovations, vol. 9, no. 1, p. bmjinnov-2021-000900, Apr. 2022, https://doi.org/10.1136/bmjinnov-2021-000900.
[42] W. Cao et al., ‘mHealth interventions for self-management of hypertension: framework and systematic review on engagement, interactivity, and tailoring’, JMIR mHealth and uHealth, vol. 10, no. 3, p. e29415, Mar. 2022, https://doi.org/10.2196/29415.
[43] N. Rachata, P. Temdee, ‘Mobile-based self-monitoring for preventing patients with type 2 diabetes mellitus and hypertension from cardiovascular complication’, Wireless Personal Communications, vol. 117, no. 1, pp. 151–175, 2021, https://doi.org/10.1007/s1127702007440w.
[44] T. Alessa, S. Abdi, M. S. Hawley, L. de Witte, ‘Mobile apps to support the self-management of hypertension: systematic review of effectiveness, usability, and user satisfaction’, JMIR mHealth and uHealth, vol. 6, no. 7, p. e10723, Jul. 2018, https://doi.org/10.2196/10723.
[45] H. Fu, S. K. McMahon, C. R. Gross, T. J. Adam, J. F. Wyman, ‘Usability and clinical efficacy of diabetes mobile applications for adults with type 2 diabetes: A systematic review’, Diabetes Research and Clinical Practice, vol. 131, pp. 70–81, 2017, https://doi.org/10.1016/j.diabres.2017.06.016.
[46] Y. Yang, H. Wang, R. Jiang, X. Guo, J. Cheng, Y. Chen, ‘A review of IoT-enabled mobile healthcare: technologies, challenges, and future trends’, IEEE Internet of Things Journal, pp. 1–1, 2022, https://doi.org/10.1109/jiot.2022.3144400.
[47] S. Zakerabasali, S. M. Ayyoubzadeh, T. Baniasadi, A. Yazdani, S. Abhari, ‘Mobile health technology and healthcare providers: systemic barriers to adoption’, Healthcare Informatics Research, vol. 27, no. 4, pp. 267–278, Oct. 2021, https://doi.org/10.4258/hir.2021.27.4.267.
[48] W. Tumuhimbise et al., ‘Maternal health-related barriers and the potentials of mobile health technologies: qualitative findings from a pilot randomized controlled trial in rural Southwestern Uganda’, Journal of Family Medicine and Primary Care, vol. 9, no. 7, p. 3657, 2020, https://doi.org/10.4103/jfmpc.jfmpc\_281\_20.
[49] M. Hamberger et al., ‘Interaction empowerment in mobile health: concepts, challenges, and perspectives’, JMIR mHealth and uHealth, vol. 10, no. 4, p. e32696, Apr. 2022, https://doi.org/10.2196/32696.
[50] A. Odeh, I. Keshta, A. Aboshgifa, E. Abdelfattah, ‘Privacy and security in mobile health technologies: challenges and concerns’, 2022 IEEE 12th Annual Computing and Communication Workshop and Conference (CCWC), Jan. 2022, https://doi.org/10.1109/ccwc54503.2022.9720863.
[51] S. Sanon, P. Temdee, ‘An agentbased detection method of condition progression trends on mobile for hypertensive diabetic patients’, in 2023 7th International Conference on Information Technology (InCIT), pp. 407–411. https://doi.org/10.1109/InCIT60207.2023.10412925.
Biographies

Sutussa Sanon, currently studying M.Sc in Digital Transformation Technology received B.Sc in Software engineering from Mae Fah Luang University. She is an entrepreneur and lead project manager on her own business in multimedia technology, previously worked as research coordinator and assistant in Mae Fah Luang University. Her research interests are multimedia technology, artificial intelligence and healthcare.

Punnarumol Temdee Ph.D. received B.Eng. in Electronics and Telecommunication Engineering, M. Eng in Electrical Engineering, and Ph.D. in Electrical and Computer Engineering from the King Mongkut’s University of Technology Thonburi. She is currently an Associate Professor at the School of Applied Digital Technology, Mae Fah Luang University, Chiang Rai, Thailand. She is also the head of Computer and Communication Engineering for Capacity Building Research Center (CCC). Her research interests are artificial intelligence and its applications, data classification, personalized learning, and personalized healthcare.
Journal of Mobile Multimedia, Vol. 21_1, 57–86.
doi: 10.13052/jmm1550-4646.2113
© 2025 River Publishers