Health Behavioral Adoption Model for Depression Intervention Using Virtual Reality Technology
Natthamol Heebjankri1, Anuchit Nirapai2 and Adisorn Leelasantitham1,*
1Technology of Information System Management Division, Faculty of Engineering, Mahidol University, NakhonPathom, Thailand
2College of Biomedical Engineering, Rangsit University, Pathum Thani, Thailand
E-mail: natthamol.hj@gmail.com; anuchit.ni@rsu.ac.th; adisorn.lee@mahidol.ac.th
Corresponding Author
Received 06 February 2025; Accepted 02 May 2025
Emotional disorders are a leading cause of suicide worldwide. Meanwhile, research has shown that Virtual Reality (VR) technology can serve as an effective intervention for emotional disorders. Therefore, this study aims to develop a health behavior model for depression intervention using VR technology. The model integrates the Health Belief Model (HBM) and the Technology Acceptance Model (TAM) and is based on data collected from 398 individuals diagnosed with depression in Suphan Buri Province, Thailand, through a structured questionnaire. Statistical analysis using Partial Least Squares Structural Equation Modeling (PLS-SEM) revealed that Perceived Usefulness (PU) had the strongest influence ( 0.448, p 0.001), followed by Perceived Ease of Use (PEOU), Perceived Barriers (PBA), Modifying Factors (MF), Cues to Action (CA), and Perceived Benefits (PBE). This study contributes theoretically by proposing a novel integration of HBM and TAM, and practically by identifying the determinants of VR technology acceptance for depression intervention. This study’s contribution facilitates the identification of the inaugural application of Modifying Factors to forecast the acceptance of VR technology, which positively influences depression intervention, thereby promoting its utilization as a therapeutic tool and enhancing emotional experiences in the future.
Keywords: Health behavior, depression, health belief model, technology acceptance model, virtual reality.
According to the World Health Organization in 2023, depression is a prevalent mental health condition, affecting more than 280 million people worldwide. It contributes to emotional disorders and increases suicide risks [1]. Therefore, providing appropriate care for individuals with depression is crucial to preventing suicide, reducing the risk of chronic depressive disorders, and facilitating their reintegration into society through functional recovery [2–4].
In the public health system, various treatment approaches are employed for depression. These include increasing general daily activities, such as exercise [5], and self-guided relaxation training. Additionally, professional interventions such as talk therapy [6], psychological therapy [7, 8] pharmacotherapy [9], and electroconvulsive therapy [10] are available. The choice of treatment depends on the severity of symptoms and may involve a single approach or a combination of methods. However, in many regions, effective treatment is hindered by a shortage of specialized mental health professionals [11] and limited awareness of available mental health treatments, particularly in low- and middle-income countries [12]. Consequently, 76–85% of individuals with depressive disorders do not receive proper treatment.
To address these challenges, technology has been increasingly integrated into depression treatment since before 2010 due to its effectiveness and cost efficiency [13, 14]. Examples include social media-based depression interventions [15]. The conceptual model is designed to combine factors from the I-Change model theory with the transtheoretical outcome of behavioral health change using social media [16], smartphone-controlled treatment processes [17], digital tools that enhance communication and coordination between patients and care teams [18], and the utilization of electronic health record data to support personalized treatment plans [19]. These technologies can enhance collaboration between patients and medical personnel and facilitate more personalized treatments based on data derived from electronic systems [19]. Notably, virtual reality (VR) technology, particularly within the Metaverse framework, has gained prominence as a tool for depression treatment and has been increasingly developed for widespread application [20]. However, despite the widespread development of such technologies in treating patients with depression [20], the use of technology-based treatments, such as Virtual Reality (VR), still lacks academic research on the acceptance models related to the treatment of emotional disorders. It is crucial to investigate the factors that both patients and caregivers encounter when using VR to ensure the technology is utilized effectively and appropriately. Therefore, this study aims to integrate (1) the Health Belief Model (HBM) [21] and (2) the Technology Acceptance Model (TAM) [22] to develop the emotional intervention acceptance model to a model designed to analyze and explain the factors influencing the acceptance of Virtual Reality (VR) technology for depression intervention to understand user behavior from both health and technology perspectives. A mixed-methods approach, combining both qualitative and quantitative methodologies, will be employed to achieve this objective.
Relying solely on health behavior theory is insufficient for studying attitude and intention factors related to users’ acceptance of VR technology. Therefore, integrating technology acceptance theory with health behavior theory is essential to ensure a comprehensive understanding of depression intervention, covering both health and technology aspects. This integration helps address research gaps and enhances the effectiveness of VR technology in depression intervention with a literature review on the theoretical frameworks used in technology acceptance for depression intervention. It highlights the significance of VR technology when applied within the context of both the Health Behavior Model (HBM) and the Technology Acceptance Model (TAM), demonstrating their combined role in shaping effective depression intervention strategies.
A literature review on the acceptance of VR technology for depression intervention highlights the growing role of Metaverse and 3D virtual world technologies in enhancing real-world environments by seamlessly integrating activities within 360-degree virtual spaces. VR technology, in particular, has been extensively developed and utilized as an intervention and treatment tool for depression, serving as an experimental platform in numerous research studies. Findings indicate that VR is highly effective and safe for depression treatment [23–25], particularly for individuals facing location, mobility, or activity limitations. VR helps bridge the gap in access to real-world experiences, offering an alternative for those confined to specific physical environments [26]. Additionally, VR has been shown to alleviate pain in patients [27]. Moreover, VR technology addresses the accessibility gap in depression treatment, providing 24/7 availability without being restricted by healthcare personnel’s working hours [28]. Self-help intervention techniques based on behavioral therapy principles have been widely adopted in depression care due to their effectiveness in reducing depressive symptoms, comparable to pharmacological treatments, while also ensuring safe usage [9]. In addition, Individuals suffering from depression have extensively employed self-help interventions within the context of behavior therapy theory due to their comparable efficacy in alleviating depression [9].
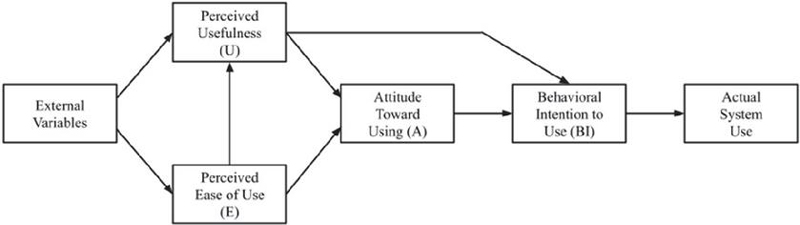
The Technology Acceptance Model (TAM) was introduced in 1986 by Fred Davis, a professor of information science and management [22], specifically to model user acceptance of information systems and technology. This model explains computer usage behavior by defining the processes that mediate the relationship between external factors and actual system use. TAM is based on the Theory of Reasoned Action (TRA), a psychological framework for understanding human behavior. By enabling users to assess their motivation for future technology adoption, TAM incorporates key factors such as external variables (technology characteristics, user demographics, and social influences), belief factors (Perceived Usefulness and Perceived Ease of Use), internal factors (Attitude Toward Using and Behavioral Intention to Use), and actual system use [29–32]. This model comprehensively reflects human cognitive psychology, making it particularly suitable for studying technology adoption among first-time users, as it clarifies the acceptance or rejection process, as illustrated in Figure 1.
Figure 1 Technology acceptance theory (TAM) [29].
The Health Belief Model (HBM) was developed in the 1950s by social scientists at the U.S. Public Health Service [33] to understand why individuals failed to adopt disease prevention strategies or participate in early-stage disease screening. Additionally, HBM has been used to examine patients’ responses to symptoms and adherence to medical treatment. It remains one of the most widely used conceptual frameworks for explaining changes in health-related behaviors and serves as a foundation for health behavior interventions. HBM is particularly valuable as it identifies individuals’ beliefs regarding (1) the perceived threat of illness or disease, (2) the influence of health behaviors based on recommendations, and (3) the likelihood of adopting health-related behaviors in the future [34–37]. The key components of HBM include modifying factors, perceived susceptibility, perceived severity, perceived threat, perceived benefits, perceived barriers, self-efficacy, and cues to action, all of which contribute to behavioral change, as illustrated in Figure 2.
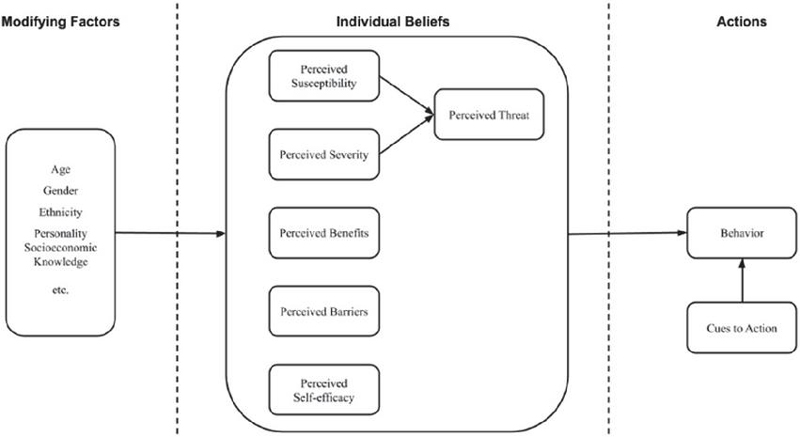
Figure 2 Health belief model [37].
This study integrates the Health Belief Model (HBM) [37] and the Technology Acceptance Model (TAM) [29] based on a comprehensive literature review to develop a conceptual framework for behavior modification using VR tools for depression prevention. The model consists of key factors and research hypotheses. The structural foundation of these theories suggests that both HBM and TAM can be categorized into four distinct groups: External Factors (e.g., Modifying Factors and External Variables), Belief Factors (e.g., Perceived Susceptibility, Perceived Threat, Perceived Severity, Perceived Benefits, Perceived Barriers, Perceived Self-Efficacy, Perceived Usefulness, and Perceived Ease of Use), Internal Factors (e.g., Attitude Toward Using and Behavioral Intention to Use), and Actions (e.g., Behavior, Cues to Action, and Actual System Use). This classification highlights the psychological mechanisms influencing behavioral change within HBM (e.g., Perceived Barriers, Modifying Factors, Perceived Benefits, and Cues to Action) while also examining the role of technology adoption in TAM (e.g., Perceived Usefulness, and Perceived Ease of Use). The structure of the framework and the interaction of its parts are shown in Figure 3.
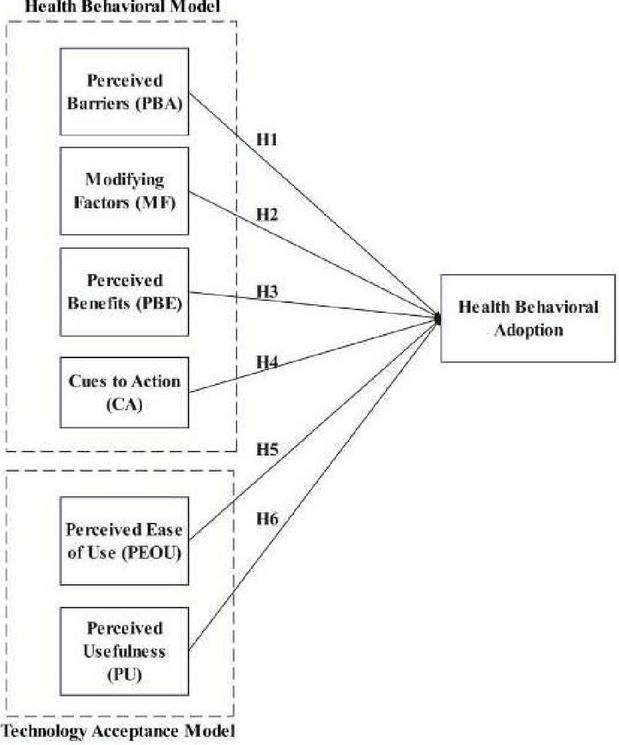
Figure 3 Research proposed model.
Perceived Barriers refer to an individual’s assessment of obstacles that may hinder health-related actions. This includes concerns about the effectiveness of a given action compared to its potential negative consequences, such as discomfort, time consumption, or inconvenience. Individuals are more likely to engage in health behaviors if they perceive these barriers as acceptable [38]. As part of the HBM framework, this factor leads to the following hypothesis:
H1: Perceived Barriers have a positive influence on the Health Behavioral Adoption Model.
Modifying Factors encompass various influences such as awareness of treatment, knowledge of disease prevention, and social background, all of which shape an individual’s perception of health behaviors [39]. As a component of HBM, this factor supports the following hypothesis:
H2: Modifying Factors have a positive influence on the Health Behavioral Adoption Model.
Perceived Benefits refer to an individual’s assessment of the effectiveness of a particular action in preventing or treating an illness. People are more likely to adopt recommended health behaviors if they perceive them as beneficial [36]. As part of HBM, this factor leads to the following hypothesis:
H3: Perceived Benefits have a positive influence on the Health Behavioral Adoption Model.
Cues to Action represent the internal or external triggers that initiate the decision-making process to adopt recommended health behaviors. Internal cues may include physical symptoms (e.g., chest pain), while external cues may involve recommendations from others or witnessing a family member’s illness [36]. As part of HBM, this factor supports the following hypothesis:
H4: Cues to Action have a positive influence on the Health Behavioral Adoption Model.
Perceived Usefulness refers to an individual’s overall evaluation of a behavior, including their beliefs about its consequences and their assessment of its benefits [40]. As a key component of TAM, this factor leads to the following hypothesis:
H5: Perceived Usefulness has a positive influence on the Health Behavioral Adoption Model.
Perceived Ease of Use is the extent to which an individual believes that using a particular system or technology will be free of effort. Behavioral intention, which reflects an individual’s willingness to adopt a behavior, is one of the strongest predictors of actual behavior [40]. As part of TAM, this factor supports the following hypothesis:
H6: Perceived Ease of Use has a positive influence on the Health Behavioral Adoption Model.
The problem, the research term, the objectives, and the literature review are all included. adoption model was introduced using factor analysis for implementing VR technology for Depression Intervention. This model, known as the Technology Adoption Model and Health Belief Model, was developed based on the study presented in Section 3. The majority of the components that make up the conceptual model.
This research employs Experimental Research to test the hypothesis in Suphan Buri province, considering the impact of the COVID-19 outbreak in 2022 on data collection and access to the sample group. The Institutional Review Board (IRB) of Bangkok delayed granting permission for field data collection, preventing public health officials in Bangkok from participating in research activities. Consequently, the researchers selected Suphan Buri province, as it was the first province authorized by the Ministry of Public Health to allow interprovincial travel. The sampling mechanism and the sample group in this study consist of a vulnerable population with limited experience using the equipment. The sample will be randomly selected from a population that meets the selection criteria, including an initial interview to verify the participants’ qualifications, with an estimated sample size of 398 individuals. Control during the VR experiment: To ensure the reliability and efficiency of the VR experiment, the researchers will control various factors, such as creating a suitable experimental environment. The VR BOX Version 2 Enhanced 3D Glasses: the material is made of ABS and PC, with a weight of 330g, which is 20 cm in length, 13.5 cm in width, and 11 cm in depth. It has a lens diameter of 42 mm. It can be accessed by Android and iOS smartphones with screens ranging from 4.5 inches to a maximum of 6 inches [41] will be used in a quiet area with sufficient lighting, and participants will receive guidance and support from village health volunteers (VHVs.) throughout the experiment to prevent stress or anxiety that may arise from using VR. The participants are going to watch the video using the YouTube app on the Amazing Thailand channel of the Tourism Authority of Thailand (TAT) by using VHS’s smartphones. The playlist consists of short video clips ranging from 0.30 to 8.00 minutes, presenting popular tourist destinations in major provinces of Thailand.
The research included questionnaires that were employed to validate the hypotheses formulated by a quantitative method to test the model, and the study’s hypotheses were adapted from validated instruments and assessed via pilot testing. Cronbach’s alpha for each construct exceeded 0.85, and AVE values surpassed 0.70, indicating high reliability. The questionnaires were employed to validate the hypotheses formulated by a quantitative method. The questionnaires included (1) demographic information such as gender, age, and education (refer to Table 1 for specifics), and (2) items formatted on a Five-level Likert Scale, where 1 denotes lowest motivation, 2 indicates low motivation, 3 represents medium motivation, 4 signifies high motivation, and 5 corresponds to highest motivation (see Table 5 for further details).
The data was acquired through a questionnaire. This study’s findings, proposed model, and underlying assumptions led to the selection of experimental research to validate the hypothesis in Suphan Buri. The Ethical Review Committee for Human Research at Mahidol University has reviewed this research and assigned it an IRB Research Project Code: COA No. MU-CIRB 2023/005.1001.
A cohort of 10 VHVs commenced data collection from a sample of 50 people in December 2022. The objective of this data collection was to evaluate the preliminary dependability of the study hypotheses and enhance its overall efficacy. The previously indicated set of research participants, having already gathered data, will refrain from recollecting data during the primary testing phase as they are categorized as VR users who do not fit the target population without prior VR experience.
In January 2023, twenty VHVs were tasked with gathering data from a sample of 398 people. The data collection method was considered successful, with no major challenges faced by the research participants.
Following the acquisition of data through a Google Form and the execution of data purification. In this data study, we utilized the SmartPLS 4.0.9.6 software to evaluate the results of the conceptual model, the structural model, and the model fit. The technique is outlined in Section 5, while Section 6 encapsulates and examines the findings derived from the data analysis and results gained by the SmartPLS program.
Table 1 Demographic data of respondents, total (N 398)
| Respondents (N =398) | |||
| Variables | Level | Frequency | Percentage |
| Gender | Male Female | 99 299 | 24.87 75.13 |
| Age | 18-20 21-30 31-40 41-20 50-60 60 | 27 56 46 240 209 | 6.78 14.07 11.56 60.30 5.03 2.26 |
| Education | Below junior high school Junior high school Senior high school Bachelor’s degree Postgraduate | 0 10 18 325 45 | 0 2.51 4.52 81.66 11.31 |
The association between variables was examined in this research using a Partial Least Squares Structural Equations Model (PLS-SEM) since it is a powerful and flexible way to examine the relationship between variables in structural data analysis or focus on the analysis of variance of data (variance-based), especially in cases where data are limited or complex, such as small data sizes, data do not meet the assumption of normal distribution, handleable multiple measured variables both reflective and formative, requires complex modeling, prediction is more important than parameter estimation, and easy to interpret, which is consistent with this study [42]. Twenty VR experiments related to the survey question outlined in Table 6 underwent statistical analysis to evaluate the reliability of the items, constructs, and hypothesis testing. Two primary components can be distinguished: a measurement model and a structural model.
A measurement model delineates the link between latent or unobserved variables MF, PBA, CA, PBE, PEOU, and PU, and observable variables MF1, MF2, MF3, PBA1, PBA2, PBA3, CA1, CA2, CA3, PBE1, PBE2, PBE3, PEOU1, PEOU2, PEOU3, PU1, PU2, and PU3. The latent variable in question is not directly measurable, yet it possesses a theoretical framework that manifests through observable behavior. This behavior can be defined via the observable variable, and its value can be calculated by employing factor analysis on a collection of observed variables that act as indicators for that variable in Table 2.
Table 2 Construct reliability and validity
| Abbr. | Measurement Items | Mean | S.D. | Loading (0.70) | Outer VIF (5.00) | Source |
| Perceived Barriers (PBA) | ||||||
| PBA1 | Is it challenging to enhance your mood when experiencing depression through the use of virtual reality? | 3.776 | 0.945 | 0.876 | 2.216 | Adapted from [45] |
| PBA2 | Do you believe that utilizing virtual reality elevates your costs? | 3.819 | 0.909 | 0.887 | 2.014 | Adapted from [46] |
| PBA3 | Does utilizing VR in nature tourism induce anxiety due to associated risks? | 3.839 | 0.905 | 0.883 | 2.293 | Adapted from [47] |
| Modifying Factors (MF) | ||||||
| MF1 | Do you believe that travel may alleviate stress? | 4.520 | 0.637 | 0.712 | 1.256 | Adapted from [48] |
| MF2 | There is an intriguing aspect to utilizing virtual reality. | 4.618 | 0.601 | 0.901 | 2.305 | Adapted from [49] |
| MF3 | Do you believe that utilizing virtual reality can benefit your health? | 4.663 | 0.551 | 0.860 | 2.196 | Adapted from [50, 51] |
| Perceived Benefits (PBE) | ||||||
| PBE1 | Do you find the use of virtual reality enjoyable? | 4.482 | 0.656 | 0.890 | 2.284 | Adapted from [52] |
| PBE2 | Do you believe that experiencing nature through virtual reality alleviates mental stress? | 4.422 | 0.689 | 0.924 | 3.150 | Adapted from [47] |
| PBE3 | Can utilizing VR to alleviate work-related fatigue safeguard your physical health against the repercussions of stress? | 4.410 | 0.761 | 0.896 | 2.621 | Adapted from [45] |
| Cues to Action (CA) | ||||||
| CA1 | Do you allow yourself to relax when you feel fatigued after work? | 4.452 | 0.660 | 0.796 | 1.542 | Adapted from [45] |
| CA2 | Does personal experience with technological devices incentivize your utilization of virtual reality? | 4.477 | 0.800 | 0.871 | 1.957 | Adapted from [53] |
| CA3 | Do different genres of trip videos inspire you to utilize virtual reality? | 4.389 | 1.299 | 0.880 | 1.967 | Adapted from [53] |
| Perceived Ease of Use (PEOU) | ||||||
| PEOU1 | I think that virtual reality is user-friendly. | 4.018 | 0.834 | 0.867 | 2.224 | Adapted from [54] |
| PEOU2 | I think it would be easy for me to use VR to alleviates mental stress. | 4.176 | 0.798 | 0.917 | 2.884 | Adapted from [54] |
| PEOU3 | The virtual reality user interface is lucid and user-friendly. | 4.138 | 0.862 | 0.903 | 2.363 | Adapted from [54] |
| Perceived Usefulness (PU) | ||||||
| PU1 | I believe that I can use VR at a critical time | 2.854 | 1.299 | 0.873 | 3.481 | Adapted from [54] |
| PU2 | I believe that utilizing virtual reality can reduce my stress awareness. | 2.905 | 1.325 | 0.851 | 3.201 | Adapted from [54] |
| PU3 | I believe I acquire valuable information from virtual reality. | 2.693 | 1.382 | 0.933 | 1.912 | Adapted from [54] |
The statistical analysis indicated a mean of 4.036, with a range of 2.693–4.663. The standard deviation (S.D.) ranged from 0.551 to 1.382, signifying a relatively minor dispersion and a negatively skewed distribution. The reliability assessment of all items yielded the subsequent outcomes: The Cronbach’s alpha () score is 0.858 show in Table 3, surpassing the acceptable level of 0.7 and exceeding the excellent criterion of 0.9 [43].
The factor loading value ranges from 0.712 to 0.924, beyond the acceptable threshold of 0.7 [43]. The Variance Inflation Factor (VIF) ranges from 1.256 to 3.481, which is below the recommended criterion of 5.00 [44]. All items demonstrated reliability surpassing the allowed criteria, as indicated in Table 2.
The model’s validity was assessed using the Fornell-Larcker criterion in accordance with the 1981 methodology. The findings, which are displayed in Table 4, demonstrate that the study model satisfies the Fornell-Larcker criterion since all of the diagonal values, which represent the square root of the AVE for each construct, were more than or equal to 0.70.
Table 3 The reliability and validity of the results
| Cronbach’s | Composite | Average Variance | ||
| Alpha | Reliability | Extracted | ||
| Constructs | Item Code | (0.70) | (CR) (0.70) | (AVE) (0.50) |
| Cues to Action | CA | 0.807 | 0.886 | 0.722 |
| Modifying Factors | MF | 0.766 | 0.867 | 0.686 |
| Perceived Usefulness | PU | 0.881 | 0.916 | 0.786 |
| Perceived Barriers | PBA | 0.858 | 0.913 | 0.778 |
| Perceived Benefits | PBE | 0.887 | 0.930 | 0.816 |
| Perceived Ease of Use | PEOU | 0.877 | 0.924 | 0.802 |
Table 4 Fornell-Larcker criterion
| Construct Name | HBM Adoption | CA | MF | PU | PBA | PBE | PEOU |
| HBM Adoption | 0.966 | ||||||
| CA | 0.696 | 0.850 | |||||
| MF | 0.339 | 0.523 | 0.828 | ||||
| PU | 0.161 | 0.123 | 0.193 | 0.886 | |||
| PBA | 0.391 | 0.385 | 0.176 | 0.082 | 0.882 | ||
| PBE | 0.742 | 0.686 | 0.386 | 0.072 | 0.364 | 0.903 | |
| PEOU | 0.734 | 0.567 | 0.341 | 0.004 | 0.596 | 0.626 | 0.896 |
A structural model is a mathematical representation that illustrates the relationships among latent or unobserved variables across various frameworks, including MF, PBA, CA, PBE, PU, and PEOU. The structural model’s measurement adheres to quality criteria, evidenced by an R2 value of 0.723, which qualifies as strong, as it surpasses the threshold of 0.67. Values below 0.19 are deemed unacceptable; those between 0.19 and 0.33 are considered weak; values from 0.33 to 0.67 are categorized as moderate; and values exceeding 0.67 are classified as strong [55]. Within the hypotheses, two are classified as intermediate (H2 and H4), while four are categorized as strong (H1, H3, H5, and H6). The study indicates that the structural model’s value exceeds the acceptable quality requirement, signifying that the quality is adequate for hypothesis testing show in Table 5 and Figure 4.
Table 5 Results of the structural model
| Path | ||||||
| Coefficient | t-value | p-value | Inner | |||
| Hypothesis | Path | () | (1.96) | (0.05) | VIF (5) | Decision |
| H1 | PBAAdoption | 0.288 | 4.961 | 0.000 | 2.353 | Supported |
| H2 | MFAdoption | 0.197 | 2.959 | 0.003 | 1.422 | Supported |
| H3 | PBEAdoption | 0.113 | 4.584 | 0.000 | 1.060 | Supported |
| H4 | CAAdoption | 0.177 | 2.671 | 0.008 | 1.590 | Supported |
| H5 | PEOUAdoption | 0.321 | 4.945 | 0.000 | 2.245 | Supported |
| H6 | PUAdoption | 0.448 | 10.858 | 0.000 | 2.291 | Supported |
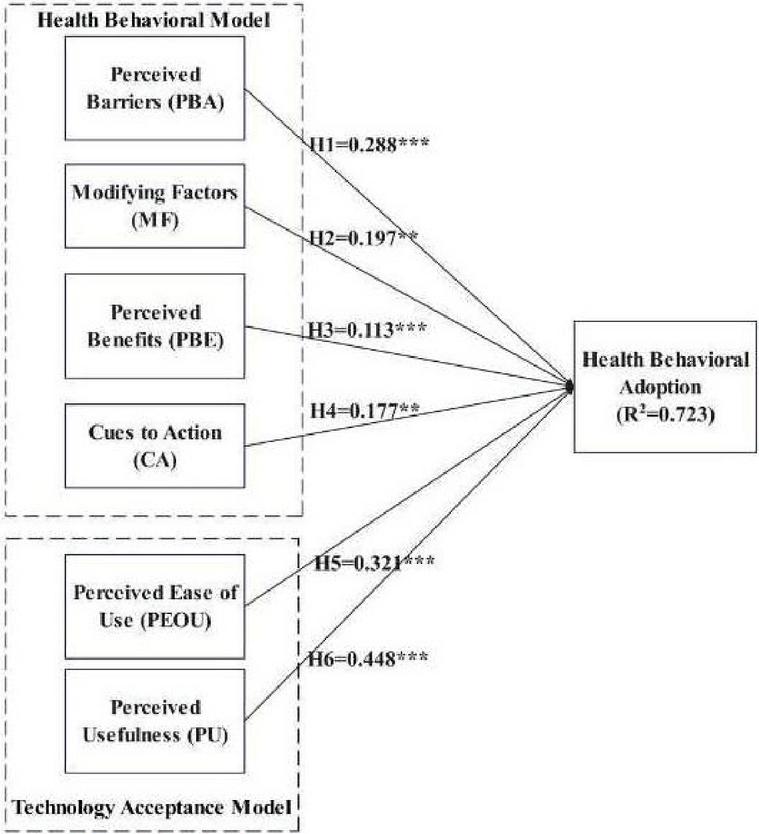
Figure 4 Summary of hypothesis testing results. *p-value 0.05; **p-value 0.01; ***p-value 0.001.
The academic contribution of this study lies in its analysis and examination of the factors influencing the acceptance behavior of VR technology for depression intervention, including Perceived Usefulness, Perceived Ease of Use, Perceived Barriers, Modifying Factors, Cues to Action, and Perceived Benefits. This research presents a novel conceptual framework for studying VR technology acceptance among individuals with mood disorders, which can serve as a foundation for teaching, learning, and future research. The findings provide valuable insights for designing tools and content for self-intervention in depression, helping to mitigate the economic burden caused by the increasing number of depressed individuals, which directly impacts healthcare budgets and patient care.
The study’s integration of HBM and TAM offers a new framework for evaluating digital mental health interventions. Comparisons with prior studies affirm the influence of PU and PEOU [29, 56]. Practical applications include designing accessible, user-friendly VR content and developing protocols for clinical use. By addressing these challenges, this research aims to support individuals in returning to normal family life. However, the study has some key limitations: (1) The researcher was unable to collect data directly due to the vulnerability of individuals with depression, requiring approval and data collection by medical personnel; (2) The COVID-19 pandemic restricted the selection of study areas. Future research can be improved by (1) incorporating additional relevant factors into the research model, (2) expanding study sites to include urban and international settings, (3) utilizing more advanced and efficient tools, and (4) exploring similar technologies such as Augmented Reality (AR), Mixed Reality (MR), or other Metaverse-based tools for comparison and validation.
The results of the study can be used to develop a new conceptual model, the process of developing a new conceptual framework, and the method of implementation by handling technology [57] for VR technology. Researchers can also use the factors they’ve gathered to look at marketing plans for the pre-purchase, purchase, and post-purchase stages of VR [58] by applying the Health Belief Model (HBM) and the Technology Acceptance Model (TAM).
Based on the statistical analysis results, the research findings indicate the order of influence of VR technology on depression intervention as follows: Perceived Usefulness, Perceived Ease of Use, Perceived Barriers, Modifying Factors, Cues to Action, and Perceived Benefits.
Perceived Usefulness is the most influential factor in VR technology acceptance for depression intervention, aligning with research on the classification of path characteristics linking health beliefs to treatment utilization in young individuals with depression [59]. This study suggests that perceived usefulness directly impacts health behavior modification.
Perceived Ease of Use ranks as the second most influential factor in VR technology acceptance for depression intervention, implying that ease of use has a direct effect on modifying health behaviors.
Perceived Barriers is the third most influential factor, consistent with research on barriers to help-seeking for depression in an Australian sample, which predicts the likelihood of future help-seeking related to depression [60]. Since individuals are generally willing to overcome obstacles to treatment when they are ill, this study suggests that if the necessary equipment is available and assistance is provided, perceived barriers to VR technology use will decrease.
Modifying Factors rank fourth in influence on VR technology acceptance for depression intervention, indicating that fundamental factors can directly impact behaviors related to depression prevention and treatment.
Cues to Action is the second-to-last influential factor, aligning with research on the classification of path characteristics linking health beliefs to treatment utilization among individuals with depression [59]. This study suggests that people with mood disorders require external stimulation to initiate decision-making processes for behavioral changes related to depression treatment.
Finally, Perceived Benefits is the least influential factor in VR technology acceptance for depression intervention. This finding is consistent with research predicting the likelihood of future help-seeking behavior for depression, which highlights that perceived treatment benefits significantly impact help-seeking intentions [60]. The study suggests that while people acknowledge benefits, without external encouragement, they may not be motivated to adopt VR technology for depression intervention.
Future studies could be improved with the following ideas: (1) adding more relevant factors into the research model, (2) extending the duration of the VR technology trial among participants, (3) diversifying the study locations, such as in cities and countries, (4) switching to more modern and efficient tools, such as Apple Vision Pro, Facebook Oculus Quest 2, HTC Vive, Sony PlayStation VR, Valve Index, and Pimax, and (5) validating it with similar technologies, such as Augmented Reality (AR) and Mixed Reality (MR), or other types of Metaverse tools.
The results of this study can be used as a guideline for creating tools and content for self-intervention in depression to reduce the impact of the gap from the shortage of health personnel and to close the economic problems caused by the impact of the depressed population, which directly affects the budget for patient care, so that they can return to normal family life.
| No. | Questions | Yes | No |
| (Over the last 2 weeks, how often have you been bothered by any of the following problems?) | |||
| 1 | Little interest or pleasure in doing things. | ||
| 2 | Feeling down, depressed, or hopeless. |
– If the answer is no to both questions, it is considered normal and not depression.
– If the answer is one or both of the following (having any symptoms in questions 1 and 2), it means “being at risk” or “likely to suffer from depression”, continue evaluating with the Depression Assessment Questionnaire (PHQ-9)
| Several | More than | Nearly | |||
| No. | Questions | Not at all | days | half the days | every day |
| (Over the last 2 weeks, how often have you been bothered by any of the following problems?) | |||||
| 0 | 1 | 2 | 3 | ||
| 1 | Little interest or pleasure in doing things. | ||||
| 2 | Feeling down, depressed, or hopeless. | ||||
| 3 | Trouble falling or staying asleep or sleeping too much. | ||||
| 4 | Feeling tired or having little energy. | ||||
| 5 | Poor appetite or overeating. | ||||
| 6 | Feeling bad about yourself or that you are a failure or have let yourself or your family down. | ||||
| 7 | Trouble concentrating on things, such as reading the newspaper or watching television. | ||||
| 8 | Moving or speaking so slowly that other people could have noticed. Or the opposite being so fidgety or restless that you have been moving around a lot more than usual. | ||||
| 9 | Thoughts that you would be better off dead, or of hurting yourself. |
| No. | Period | Questions | No Have | Have |
| 1 | Have you wanted to die, or do you think it would be better to die? | 0 | 1 | |
| 2 | Have you wanted to hurt yourself or injure yourself? | 0 | 2 | |
| 3 | During the past 1 month, including today. | Have you been thinking about suicide? | 0 | 6 |
| (If you answer that you are thinking about committing suicide, ask further.) Can you be able to control the suicidal thoughts you are thinking about? Or can you tell me that you probably will not act on those thoughts at this time? | Can 0 | Can not 8 | ||
| 4 | Have you planned to commit suicide? | 0 | 8 | |
| 5 | Have you prepared to harm yourself or prepared to commit suicide with the intention of actually dying? | 0 | 9 | |
| 6 | Have you have injured yourself but did not intend to cause death? | 0 | 4 | |
| 7 | Have you have attempted suicide expecting/intending to die? | 0 | 10 | |
| 8 | Throughout the past life. | Have you ever tried to commit suicide? | 0 | 4 |
| Total Score | Suicide Severity |
| 0 | No suicidal tendency. |
| 1–8 | Mild tendency to commit suicide. |
| 9–16 | Moderate tendency to commit suicide. |
| ≥17 | Severe tendency to commit suicide. |
| Remark: If the total score is greater than equal to 17, immediately refer to a hospital with a psychiatrist. | |
[1] Millner A, Den Ouden H, Gershman S, Glenn C, Kearns J, Bornstein A, et al. Suicidal thoughts and behaviors are associated with an increased decision-making bias for active responses to escape aversive states. Journal of Abnormal Psychology. 2019; 128(2): 106. https://doi.org/10.1037/abn0000395.
[2] Doupnik SK, Rudd B, Schmutte T, Worsley D, Bowden CF, McCarthy E, et al. Association of suicide prevention interventions with subsequent suicide attempts, linkage to follow-up care, and depression symptoms for acute care settings: a systematic review and meta-analysis. JAMA Psychiatry. 2020; 77(10): 1021–1030. https://doi.org/10.1001/jamapsychiatry.2020.1586.
[3] Torok M, Han J, Baker S, Werner-Seidler A, Wong I, Larsen ME, et al. Suicide prevention using self-guided digital interventions: a systematic review and meta-analysis of randomised controlled trials. Lancet Digit Health. 2020; 2(1): e25–e36. https://doi.org/10.1016/S2589-7500(19)30199-2.
[4] Katz C, Bolton SL, Katz LY, Isaak C, Tilston-Jones T, Sareen J; Swampy Cree Suicide Prevention Team. A systematic review of school-based suicide prevention programs. Depression and Anxiety. 2013; 30(10): 1030–1045. https://doi.org/10.1002/da.22114.
[5] Dorow M, Löbner M, Pabst A, Stein J, Riedel-Heller SG. Preferences for depression treatment including internet-based interventions: results from a large sample of primary care patients. Frontiers in Psychiatry. 2018; 9: 181. https://doi.org/10.3389/fpsyt.2018.00181.
[6] Christensen H, Griffiths KM, Jorm AF. Delivering interventions for depression by using the internet: randomised controlled trial. BMJ. 2004; 328(7434): 265. https://doi.org/10.1136/bmj.37945.566632.EE.
[7] Patel V, Weobong B, Weiss HA, Anand A, Bhat B, Katti B, et al. The Healthy Activity Program (HAP), a lay counsellor-delivered brief psychological treatment for severe depression, in primary care in India: a randomised controlled trial. Lancet. 2017; 389(10065): 176–185.
[8] Cuijpers P, Quero S, Dowrick C, Arroll B. Psychological treatment of depression in primary care: recent developments. Current Psychiatry Reports. 2019; 21(12): 129. https://doi.org/10.1007/s11920-019-1117-x.
[9] Karrouri R, Hammani Z, Benjelloun R, Otheman Y. Major depressive disorder: validated treatments and future challenges. World J Clin Cases. 2021; 9(31): 9350–9367. https://doi.org/10.12998/wjcc.v9.i31.9350.
[10] Black DW, Winokur G, Nasrallah A. The treatment of depression: electroconvulsive therapy antidepressants: a naturalistic evaluation of 1,495 patients. Comprehensive Psychiatry. 1987; 28(2): 169–182. https://doi.org/10.1016/0010-440X(87)90082-4.
[11] Cummings JR, Zhang X, Gandré C, Morsella A, Shields-Zeeman L, Winkelmann J, et al. Challenges facing mental health systems arising from the COVID-19 pandemic: evidence from 14 European and North American countries. Health Policy. 2023; 136: 104878. https://doi.org/10.1016/j.healthpol.2023.104878.
[12] Sorsdahl K, Petersen I, Myers B, Zingela Z, Lund C, van der Westhuizen C. A reflection of the current status of the mental healthcare system in South Africa. SSM – Mental Health. 2023; 4: 100247. https://doi.org/10.1016/j.ssmmh.2023.100247.
[13] Newman MG, Szkodny LE, Llera SJ, Przeworski A. A review of technology-assisted self-help and minimal contact therapies for anxiety and depression: is human contact necessary for therapeutic efficacy? Clinical Psychology Review. 2011; 31(1): 89–103. https://doi.org/10.1016/j.cpr.2010.09.008.
[14] Hay JW, Lee PJ, Jin H, Guterman JJ, Gross-Schulman S, Ell K, et al. Cost-effectiveness of a technology-facilitated depression care management adoption model in safety-net primary care patients with type 2 diabetes. Value in Health. 2018; 21(5): 561–568. https://doi.org/10.1016/j.jval.2017.11.005.
[15] Plackett R, Blyth A, Schartau P. The impact of social media use interventions on mental well-being: systematic review. Journal of Medical Internet Research. 2023; 25: e44922. https://doi.org/10.2196/44922.
[16] Nusawat P, Leelasantitham A. A new consistent concept between the I-change Model and the Transtheoretical Outcome to imply the leading guideline of depression behavior health change using social media. Open Public Health Journal, 2024; 17: e18749445318733. http://dx.doi.org/10.2174/0118749445318733240513061523.
[17] Serrano-Ripoll MJ, Zamanillo-Campos R, Fiol-DeRoque MA, Castro A, Ricci-Cabello I. Impact of smartphone app-based psychological interventions for reducing depressive symptoms in people with depression: systematic literature review and meta-analysis of randomized controlled trials. JMIR mHealth and uHealth. 2022; 10(1): e29621. http://dx.doi.org/10.2196/29621.
[18] Walsh AEL, Naughton G, Sharpe T, Zajkowska Z, Malys M, van Heerden A, et al. A collaborative realist review of remote measurement technologies for depression in young people. Nature Human Behaviour. 2024; 8: 480–492. https://doi.org/10.1038/s41562-023-01793-5.
[19] Nickson, D, Meyer, C, Walasek, L, Toro, C. Prediction and diagnosis of depression using machine learning with electronic health records data: a systematic review. BMC Medical Informatics and Decision Making. 2023; 23(1): 271. https://doi.org/10.1186/s12911-023-02341-x.
[20] Paul M, Bullock K, Bailenson J. Virtual reality behavioral activation for adults with major depressive disorder: feasibility randomized controlled trial. JMIR Ment Health. 2022; 9(5): e35526. https://doi.org/10.2196/35526.
[21] Albert KM, Newhouse PA. Estrogen, Stress, and Depression: Cognitive and Biological Interactions. Annual Review of Clinical Psychology. 2019; 15: 399–423. https://doi.org/10.1146/annurev-clinpsy-050718-095557.
[22] Venkatesh V, Morris MG, Davis GB, Davis FD. User acceptance of information technology: toward a unified view. MIS Quarterly. 2003; 27(3): 425–478. https://doi.org/10.2307/30036540.
[23] Ioannou A, Papastavrou E, Avraamides MN, Charalambous A. Virtual reality and symptoms management of anxiety, depression, fatigue, and pain: a systematic review. SAGE Open Nursing. 2020; 6: 2377960820936163. https://doi.org/10.1177/2377960820936163.
[24] Jingili N, Oyelere SS, Ojwang F, Agbo FJ, Nyström MBT. Virtual reality for addressing depression and anxiety: a bibliometric analysis. International Journal of Environmental Research and Public Health. 2023; 20(9): 5621. https://doi.org/10.3390/ijerph20095621.
[25] du Plessis J, Jordaan J. The impact of virtual reality on the psychological well-being of hospitalised patients: A critical review. Heliyon. 2024; 10(2): e24831. https://doi.org/10.1016/j.heliyon.2024.e24831.
[26] Creed C, Al-Kalbani M, Theil A, Sarcar S, Williams I. Inclusive Augmented and Virtual Reality: A Research Agenda. International Journal of Human–Computer Interaction. 2024; 40(20): 6200-6219. https://doi.org/10.1080/10447318.2023.2247614.
[27] Li A, Montaño Z, Chen VJ, Gold JI. Virtual reality and pain management: current trends and future directions. Pain Management. 2011; 1(2): 147–157. https://doi.org/10.2217/pmt.10.15.
[28] Kim S, Kim E. The use of virtual reality in Psychiatry: a review. Journal of the Korean Academy of Child and Adolescent Psychiatry. 2020; 31(1): 26–32. https://doi.org/10.5765/jkacap.190037.
[29] Davis FD. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Quarterly. 1989; 13(3): 319–340. http://dx.doi.org/10.2307/249008.
[30] Goodhue DL. Comment on Benbasat and Barki’s “Quo Vadis TAM” article. Journal of the Association for Information Systems. 2007; 8(4). https://doi.org/10.17705/1jais.00125.
[31] Rauniar R, Rawski G, Yang J, Johnson B. Technology acceptance model (TAM) and social media usage: an empirical study on Facebook. Journal of Enterprise Information Management. 2014; 27(1): 6–30. https://doi.org/10.1108/JEIM-04-2012-0011.
[32] Nirapai A, Leelasantitham A. A new adoption model for quality of experience assessed by radiologists using AI medical imaging technology. Journal of Open Innovation: Technology, Market, and Complexity. 2024; 10(3): 100369. https://doi.org/10.1016/j.joitmc.2024.100369.
[33] Becker MH. The health belief model and personal health behavior. Health Education Monographs. 1974; 2: 324–508. http://dx.doi.org/10.1177/109019817400200407.
[34] Rosenstock IM, Strecher VJ, Becker MH. Social learning theory and the Health Belief Model. Health Education Quarterly. 1988; 15(2): 175–183. https://doi.org/10.1177/109019818801500203.
[35] Champion VL, Skinner CS. The Health Belief Model. In: Health Behavior and Health Education: Theory, Research, and Practice. 4th ed. San Francisco: Jossey-Bass; 2008. 45–65.
[36] LaMorte WW. The Theory of Planned Behavior, The Social Cognitive Theory, The Health Belief Model. Boston University School of Public Health; [cited 2025 Apr 21]. Available from: https://courses.lumenlearning.com/suny-hvcc-healthpsychology/chapter/changing-health-habits.
[37] Zewdie HY, Whetten K, Dubie ME, Kenea B, Bekele T, Temesgen C, et al. The association between urban greenspace and psychological health among young adults in Addis Ababa, Ethiopia. Environmental Research. 2022; 215(Pt1): 114258. https://doi.org/10.1016/j.envres.2022.114258.
[38] Ghorbani-Dehbalaei M, Loripoor M, Nasirzadeh M. The role of health beliefs and health literacy in women’s health promoting behaviours based on the health belief model: a descriptive study. BMC Women’s Health. 2021; 21: 421. https://doi.org/10.1186/s12905-021-01564-2.
[39] Kalua F, Nyasulu Y. A review of the role of modifying factors in health education programmes. Malawi medical journal: the journal of Medical Association of Malawi. 2007; 19(1): 30-31. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3615310/.
[40] Fishbein M, Ajzen I. Belief, Attitude, Intention, and Behavior: An Introduction to Theory and Research. Reading, MA: Addison-Wesley; 1975. ISBN-10: 0201020890.
[41] Primecables. VR BOX v.2 Enhanced VR headset virtual reality 3D glasses. Primecables; 2024 [cited 2024 Feb 11]. Available from: https://www.primecables.ca/p-357058-cab-03017-all-vr-box-v2-enhanced-vr-headset-virtual-reality-3d-glasses?fbclid=IwAR1CPGdbXK7mPYzDRQ1pOI6eClEE8NLkOc6u4HNlJOm7LicFC2gckl2YLLU\#sku365386.
[42] Urbach N, Ahlemann F. Structural equation modeling in information systems research using partial least squares. Journal of Information Technology Theory and Application. 2010; 11(2): 5–40. Available from: https://aisel.aisnet.org/jitta/vol11/iss2/2.
[43] Hair JF Jr, Matthews LM, Matthews RL, Sarstedt M. PLS-SEM or CB-SEM: updated guidelines on which method to use. International Journal of Multivariate Data Analysis. 2017; 1(2): 107–123. https://dx.doi.org/10.1504/IJMDA.2017.087624.
[44] Ringle CM, Wende S, Becker J-M. SmartPLS 3. Boenningstedt: SmartPLS GmbH; 2015. Available from: https://www.researchgate.net/publication/270883448\_SmartPLS\_3.
[45] Okechukwu C, Babatunde OB. Work-related stress and the relationship with the Health Belief Model among medical doctors in a Tertiary Hospital in Port-Harcourt, Nigeria. Journal of Education, Society and Behavioural Science. 2021; 34(4): 10–21. https://doi.org/10.9734/jesbs/2021/v34i430320.
[46] Nexøe J, Kragstrup J, Søgaard J. Decision on influenza vaccination among the elderly. A questionnaire study based on the Health Belief Model and the Multidimensional Locus of Control Theory. Scandinavian Journal of Primary Health Care. 1999; 17(2): 105–110. https://doi.org/10.1080/028134399750002737.
[47] Jeong JY, Lee K-Y. A rebound in nature-based tourism intentions during the COVID-19 era. Journal of Vacation Marketing. 2023; 29(4): 636–653. https://doi.org/10.1177/13567667221111566.
[48] Zhou C, McCarthy SA, Durbin R. YaHS: yet another Hi-C scaffolding tool. Bioinformatics. 2023; 39(1): btac808. https://doi.org/10.1093/bioinformatics/btac808.
[49] Santos Garduño HA, Esparza Martínez MI, Portuguez Castro M. Impact of virtual reality on student motivation in a high school science course. Applied Sciences. 2021; 11(20): 9516. https://doi.org/10.3390/app11209516.
[50] Jattamart A, Leelasantitham A. Perspectives to social media usage of depressed patients and caregivers affecting to change the health behavior of patients in terms of information and perceived privacy risks. Heliyon. 2020; 6(6): e04244. https://doi.org/10.1016/j.heliyon.2020.e04244.
[51] Jattamart A, Leelasantitham A. The influence of social media lifestyle interventions on health behaviour: a study on patients with major depressive disorders and family caregivers. The Open Public Health Journal, 2019; 12. http://dx.doi.org/10.2174/1874944501912010387.
[52] Abu-Taieh EM, AlHadid I, Masa’deh R, Alkhawaldeh RS, Khwaldeh S, Alrowwad A. Factors Affecting the Use of Social Networks and Its Effect on Anxiety and Depression among Parents and Their Children: Predictors Using ML, SEM and Extended TAM. International Journal of Environmental Research and Public Health. 2022 Oct;19(21):13764. https://doi.org/10.3390/ijerph192113764.
[53] Yuen KF, Koh LY, Tan LYH, Wang X. The determinants of virtual reality adoption for marine conservation. Technology in Society. 2023; 72: 102170. https://doi.org/10.1016/j.techsoc.2022.102170.
[54] Venkatesh V, Thong JYL, Xu X. Consumer acceptance and use of information technology: extending the Unified Theory of Acceptance and Use of Technology. MIS Quarterly. 2012; 36(1): 157–178. https://doi.org/10.2307/41410412.
[55] Chin WW, Marcoulides G. The partial least squares approach to structural equation modeling. In: Marcoulides GA, editor. Modern Methods for Business Research. Mahwah, NJ: Lawrence Erlbaum Associates; 1998. 311–336. Available from: https://www.researchgate.net/publication/311766005\_The\_Partial\_Least\_Squares\_Approach\_to\_Structural\_Equation\_Modeling.
[56] Yang HJ, Lee JH, Lee W. Factors influencing health care technology acceptance in older adults based on the technology acceptance model and the unified theory of acceptance and use of technology: meta-analysis. Journal of Medical Internet Research. 2025; 27: e65269. https://doi.org/10.2196/65269.
[57] Leelasantitham A. A novel guideline framework for research and development in the field of management of technology and innovation. In: 2024 5th Technology Innovation Management and Engineering Science International Conference (TIMES-iCON), Bangkok, Thailand, 2024. Piscataway, NJ: IEEE; 2024. 1–5. https://doi.org/10.1109/TIMES-iCON61890.2024.10630775.
[58] Puengwattanapong P, Leelasantitham A. A holistic perspective model of plenary online consumer behaviors for sustainable guidelines of the electronic business platforms. Sustainability. 2022; 14(10): 6131. https://doi.org/10.3390/su14106131.
[59] Lilly FR, Jun HJ, Alvarez P, Owens J, Malloy L, Bruce-Bojo M, et al. Pathways from health beliefs to treatment utilization for severe depression. Brain and Behavior. 2020;10(12): e01873. https://doi.org/10.1002/brb3.1873.7.
[60] Langley EL, Wootton BM, Grieve R. The utility of the Health Belief Model variables in predicting help-seeking intention for anxiety disorders. Australian Psychologist. 2018; 53(4): 291–301. https://doi.org/10.1111/ap.12334.

Natthamol Heebjankri earned a Bachelor of Science in Computer Science from Phranakhon Rajabhat University in 2005 and a master’s degree in computer and information technology from King Mongkut’s University of Technology Thonburi (KMUTT), Thailand, in 2008. She is currently an Assistant Professor in the Department of Technology and Data Science, Faculty of Science and Technology, Bansomdejchaopraya Rajabhat University, Thailand. In this role, she teaches courses in Data Analysis, Information Technology Management, and Data Science.

Anuchit Nirapai received Bachelor of Science in Communication Engineering from Srinakharinwirot University, his Master of Science in Communication Engineering from King Mongkut’s University of Technology North Bangkok, and his Doctor of Philosophy program in Information Technology Management from Mahidol University Thailand in 2008, 2015, and 2023, respectively. Presently, he holds a position as a lecturer in the College of Biomedical Engineering at Rangsit University. In this role, he instructs courses on software design, health information technology, information technology management, and the Internet of Medical Things (IoMT).

Adisorn Leelasantitham received the B.Eng. degree in Electronics and Telecommunications and the M.Eng. degree in Electrical Engineering from King Mongkut’s University of Technology Thonburi (KMUTT), Thailand, in 1997 and 1999, respectively. He received his Ph.D. degree in Electrical Engineering from Sirindhorn International Institute of Technology (SIIT), Thammasat University, Thailand, in 2005. He is currently the Associate Professor in Technology of Information System Management Division, Faculty of Engineering, Mahidol University, Thailand. His research interests include applications of blockchain technology, conceptual models and frameworks for IT management, disruptive innovation, image processing, AI, neural networks, machine learning, IoT platforms, data analytics, chaos systems, and healthcare IT. He is a member of the IEEE.
Journal of Mobile Multimedia, Vol. 21_2, 245–274.
doi: 10.13052/jmm1550-4646.2123
© 2025 River Publishers