Effectiveness of Contact Tracing Using KNN for COVID-19
Maheshwari Venkatasen1,*, Sandeep Kumar Mathivanan1, Prasanna Mani1, Prabhu Jayagopal1, Thanapal P1, Manivannan Sorakaya Somanathan1, Upendra Babu K2 and Elangovan D3
1School of Information Technology and Engineering, Vellore Institute of Technology, Vellore, TamilNadu, India
2Computer Science and Engineering, JNN Institute of Engineering, Chennai, TamilNadu, India
3Computer Science and Engineering, Panimalar Engineering College, Chennai, TamilNadu, India
E-mail: maheshwarivenkat24@gmail.com
*Corresponding Author
Received 26 April 2021; Accepted 19 May 2021; Publication 18 June 2021
Abstract
COVID-19 virus started to outbreak in China in the year January 2020. Contact tracing is an open-minded measure of control that applies to an extensive range of transmissible diseases. It is being used to fight infections like SARS, tuberculosis, smallpox, and many sexually transmitted diseases (STDs). From the moment of the lockdown, there have been a great many talks of applications helping to combat the coronavirus. Technical developers bring a solution to this problem by providing tools that help to contain the coronavirus. This kind of application is helpful, but it lacks in accuracy and privacy concerns. COVID-19 virus, irrespective of causes, solution, treatments, clinical signs, and symptoms is discussed in this paper. The main aim of this paper proposes a contact tracing using k-nearest neighbour, which shows the correct prediction of an affected person of COVID-19 based on the distance and also reduces the transmission of disease. It was tested on the WHO dataset obtained the prediction accuracy of which was carried out on clinical and quarantine data. The evaluation result shows that the contact tracing technique’s accuracy has been improved using the proposed algorithm.
Keywords: COVID-19, Contact tracing, k-nearest neighbour, World Health Organization (WHO).
1 Introduction
The World Health Organisation (WHO) reports that infectious viruses remain to evolve and significant concern to people’s well-being. Many virus pandemics were reported over the past 20 years, namely Serious Acute Respiratory Syndrome (SARS-COV) from 2002 to 2003 and H1N1 influenza in 2009. The Middle East respiratory syndrome coronavirus (MERS-COV) was first found in Saudi Arabia in 2012 [1].COVID-19 is an airborne infection triggered by extreme acute or chronic syndrome. The syndrome was originally reported in Wuhan (China), in Dec 2019. The research report can track the starting of symptomatic persons back to the starting of December 2019. The first cases were labeled as “pneumonia of unknown etiology” because unable to find the causative agents [1]. Advanced epidemic studies were conducted through the center for disease control and prevention. This disease’s causative agents are now referred to as a new virus fit into the coronavirus (COV) family. According to the report on February 11, 2020, the WHO director-stated that the condition affected through a novel COV was a “COVID-19”, acronyms with the “coronavirus disease 2019” [2]. Two new corona-virus outbreaks have occurred over the past 20 years. SARS-COV triggered a broad-ranging spread origination in china involving two dozen nations around 8,000 cases and 800 deaths, and MERS-COV started in Saudi Arabia and around 2,500 cases and 800 deaths and still affects sporadic cases. This new virus appears incredibly viral, and it has spread throughout the world [2]. On January 30, 2020, the epidemic was announced by the WHO as a Public Health Emergency International Concern (PHEIC) following International Health Regulations (IHR, 2005) as the epidemic has extended to nearly 18 countries, with four countries indicating that human to human transmission [3]. On February 26, 2020, a further breakthrough happened, when the first outbreak of the disease, not imported from China, was identified in the US. The new virus was initially named 2019-nCOV [4]. The task of scientists at the International Committee on Taxonomy of Viruses (ICTV) was eventually labeled as the SARS-COV-2 virus because it is very close to the individual that leads to a SARS epidemic (SARS-COVs).COVs are the key pathogen of an emerging respiratory disease epidemic. They are a large family of RNA viruses with single-stranded (ssRNA), which can be found in various animal species [5]. For purposes that still have to be addressed, this virus can cross the species barrier and spread diseases to people, infection varying from the cold or flu too much severe diseases like SARS and MERS. Surprisingly, this latter pathogen is defined by bats and moved into other mammal species, Himalayan palm civet for SARS-COV and the dromedary camel for MERS-COV before switching humans [6]. There is no knowledge about the nature of SAR-COV-2, but there is evidence that it also originated from animals. The possibility of such viruses evolving worldwide into a disease outbreak is a serious risk to human health. The impact of the epidemic triggered by the new COV is likely, still growing as the condition develops quickly.
World governments are working on protective measures to counteract the destructive consequences. Health organization manages the flow of information and problems instructions to reduce the effects of the risk. Simultaneously, scientists worldwide are working relentlessly, and information is rapidly evolving about the transmission process, clinical range, new diagnostics, mitigation, and therapeutic approaches. There are several suspicions involving the nature of the virus-host and the virus’s growth, especially when the epidemic will reach its level. Currently, medical approaches to work with infection are only supportive, and the best resources are prevention to decrease transmission in society [1].
2 COVID-19 Virus: Impact, Symptoms, Solution, Isolation Period, Treatments
2.1 Impacts Of COVID-19
The virus spreads predominantly through physical contact by tiny droplets released during cough, sneezing, or talking. Such small droplets can be generated through breathing, but the virus usually is not spread by air. People can also get infected by touching the surface and their faces. The virus can thrive in environments for up to 72 hours [7]. It is peak activity in the initial three-day before the arrival of symptoms, but the infection can transmit before and in the middle stages of development. The duration of reaction to symptoms typically differs from 2 to 14 days and is now on a maximum of 5 days [7]. The typical analysis method is by real-time reverse transcription-polymerase chain reaction (Rrt-PCR) from a nasopharyngeal swab. The contamination might be treated with several symptoms, medical conditions, and chest CT scans with pneumonia features.
The COVID-19 virus impact, symptoms, solution, isolation period, and treatments are shown in Figure 1.
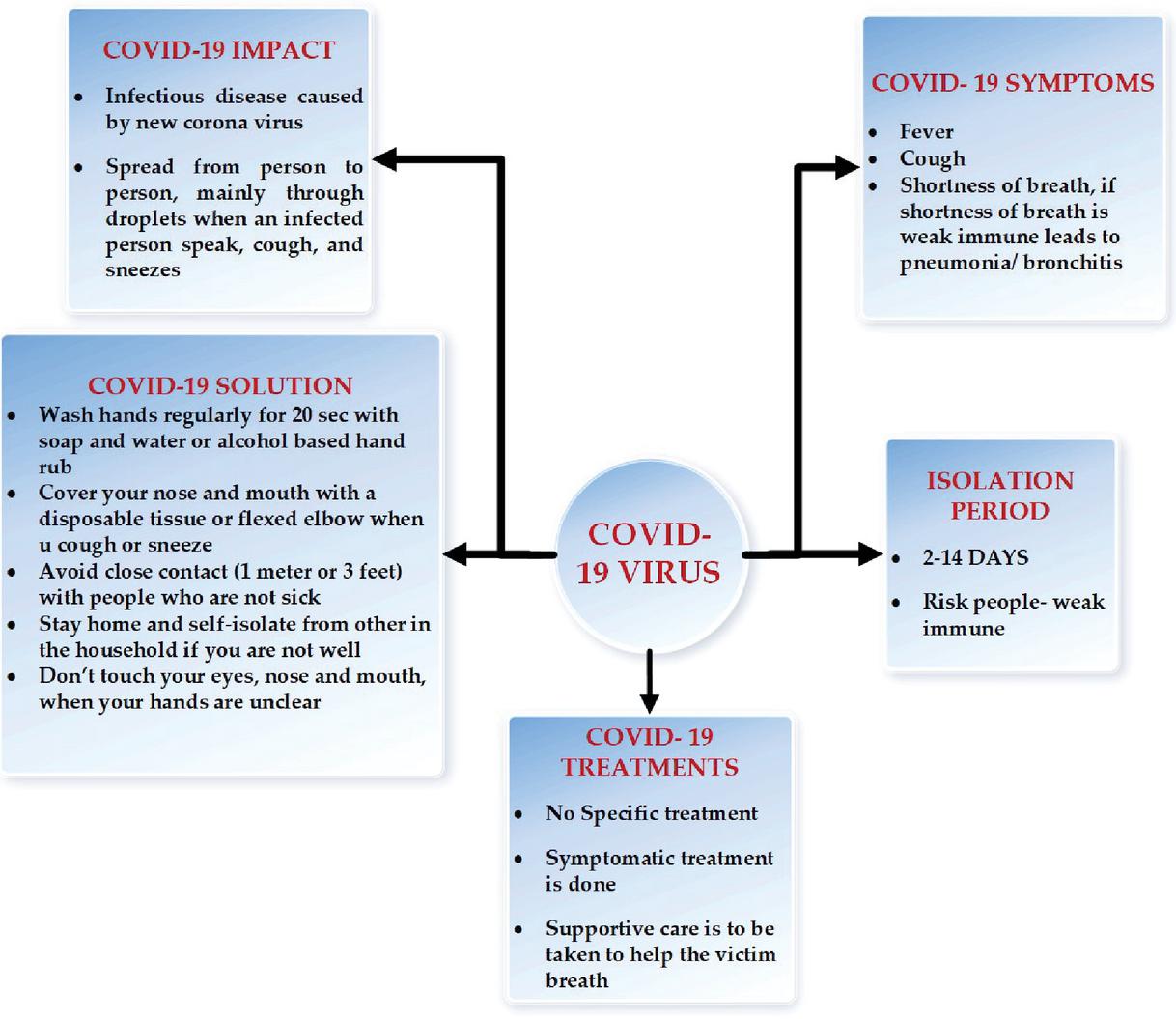
Figure 1 COVID-19 virus: clinical signs, symptoms, solution and treatments.
2.2 Sign and Symptoms Of COVID-19
Infected people by the virus can experience asymptomatic or flu-like complications like fever, cough, tiredness, and chest pain [8]. Immediate indications involve difficulty in breathing and waking, constant chest pain; medical care must be provided promptly if all those symptoms occur [9]. Upper respiratory complaints like sneezing, sore throat, or sore neck are quite frequently observed. In specific scenarios, china originally presented only with palpitation and chest pain. In March 2020, there were confirmed that loss of the sense of anosmia could remain a common symptom for those with mild diseases, while not as common as it was initially recorded. In some diseases can evolution to pneumonia, multi-organ failure, and death. For individuals with severe signs, time from symptom inception requires mechanical ventilation up to 8 days [10]. There is a gap among the time and person is infected with the virus and the period when they built indications. It recognized as the period of incubation. The incubation duration usually has 5 to 6 days, although it can be from 2 to 14 days. 97.5% of people with signs can use it within 11.5 days of contagion [11]. The reports suggest this not all infected people experience symptoms, but their involvement in the spread is unknown. Recent data recommend that asymptomatic cases might lead to the transmission of the virus. The symptoms and occurred percentage of COVID-19 is shown in Figure 2.
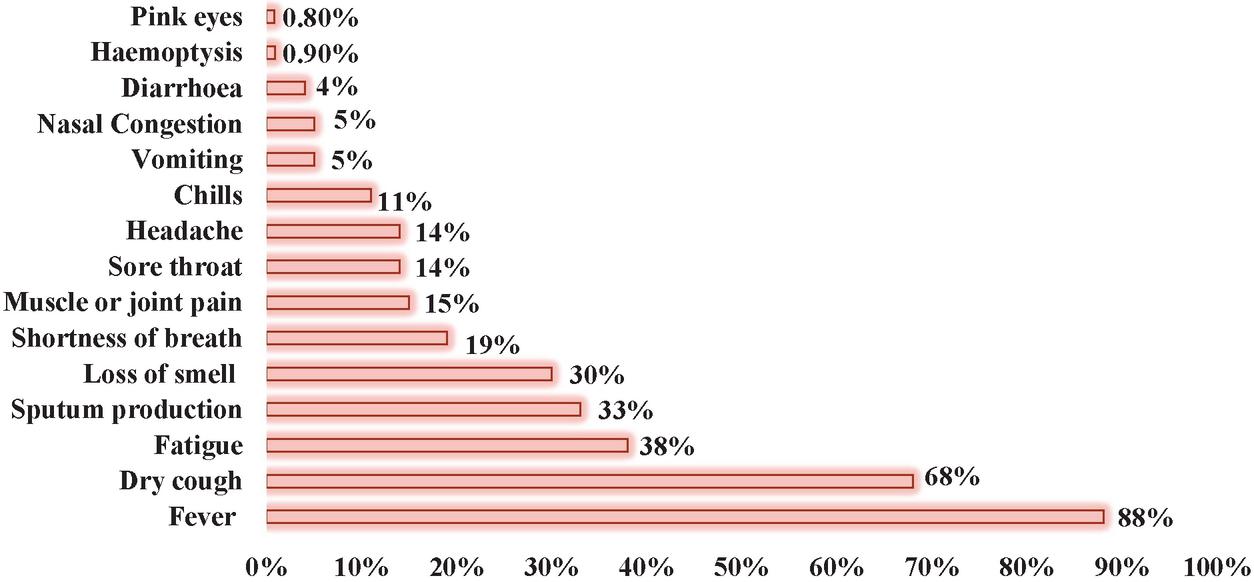
Figure 2 Symptoms and occurred percentage of COVID-19.
2.3 Prevention of COVID-19
Prevention efforts to minimize infection chances mean staying indoors, avoiding traffic places, handwashing often for at least 20 seconds with soap, and examining good respiratory hygiene [12, 13]. Centers for Disease Control and Prevention (CDC) advise cover the mouth and nose with a tissue; when coughing or sneezing and prescribes to use inner elbow if the tissue is not available [12]. The social distancing approaches limit interaction between infected people with large numbers by lockdown the colleges and offices, decreasing travel, and postponing the mass gathering [14]. Social distance implies that the public should stay at least six feet away from the people. As a vaccine is not expected to occur until 2021 [15], a core measure of controlling COVID-19 is attempted to reduce outbreak level known as flattening the curve [16]. It’s accomplished by slowing down the amount of infection to mitigate the risk that healthcare facilities will be overloaded, permit improved treatment to present cases, and delay more infection cases till suitable medications or vaccines are affordable [17].
World health organization (WHO), mask usage is one suggested if individual coughs or sneezes or takes care of a person with suspected infection [18]. China, Hong Kong, Thailand, and Austria suggested wearing masks for healthy individuals [19]. The WHO predicts that global demand will increase by 40% to achieve the necessity of masks. The problem has been worsened by hunting and speculation; the cost of masks climbed six times, N95 respirators tripled, and gowns doubled [20]. Most of the expertise in health care suggested that wearing a non-medical mask, as well as other face coverings such as scarves or bandanas, are an excellent technique to protect from the public, whoever touches their mouth and noses, even though non-medical covering does not shield against natural cough or sneezing from the affected person [21].
2.4 Treatment of COVID-19
There is no prescribed antiviral treatment suggested for COVID-19, and currently, no vaccine affordable. The diagnosis is symptomatic, and oxygen therapy is the leading recovery protocol for severe infection cases [1]. Mechanical ventilation may be necessary for refractory oxygen therapy in respiratory failure, while neurologic assistance is vital in treating septic shock. As per a report on January 28, 2020, the world health organization issued a document outlining that suggested and provided guidance for treating past disease outbreaks from the Co-circulation of four Human Coronaviruses (HCOVs). This document explores steps to identify and sort out patients with Severe Acute Respiratory Disease (ARDs), prevention of infections and control strategies, early supportive therapy and monitoring, rules for laboratory diagnosis, control of respiratory failure and ARDS, prevention of septic shock, treatments, and precautions for pregnant patients. These guidelines incorporate methods for adapting to respiratory failure, namely mechanical safety ventilation and High-Flow Nasal Oxygen (HFNO) [22].
2.5 Contact Tracing Via Smartphone App
Contact tracing software will secure confidential user data and also faces counter feedback [23]. The list of contact tracing applications using in European countries is listed below.
2.6 Next-Step app
The SBB app developers have developed the Next-Step app to help people out of the corona crisis. Next-step app support android 6.0 or higher version, and its coverage of about 95 percent of android devices in Switzerland than in the world. During self-quarantine, this app mainly focused on the principles of a person’s accountability and unity. Therefore, we hope that the user will follow the same way and be mindful of the impact of wrong information.
2.7 PEPP-PT App
PEPP-PT app is a European contact tracing app. This technology is based on Bluetooth-based proximity technology. Every minute, this app creates a new token exchanged through Bluetooth. Different tokens are generated if the same person available to someone for a long-time. It does not support the ios version. Accuracy of data is encountered about the 15-meter distance of devices. Encrypted data are being protected; sensitive data are not stored. But data are currently deleted within 14 days on server and clients because it is no longer critical to track contacts.
2.8 ALERTSWISS app
It is developed by ambique. It is almost installed in six lakh mobile devices and makes it easy for the government for contact tracing.
3 Literature Review
During 1918, influenza-infected people spread the virus among 1 and 2 of their social contacts [24]. The same refers to those quarantined with the Ebola virus in the 2014 epidemic in West Africa [25, 26]. However, the Ebola infection impacted a 10:1 percentage of the number of people estimated to be affected by the 1918 influence virus [27, 28]. Enhancements in health care, public health care, and human psychology change partially compensate for the significant difference between Ebola in 2014 and influenza in 1918 [29]. The considerable variance among viruses, namely the variability of a single infected person in the number of secondary cases. Hebert-Dufresne et al. (2020) demonstrate the numerical significance of measuring the variability in the amount of secondary infection through contact tracking for evaluating the risk of infection in new pathogens [30].
The primary public safety response to the import of new and emerging pathogens involved contact tracking applied in the UK for the period of the control phase of influenza or flu plague in 2009 [31].In latest times, contact tracking has become vital resource since, after importing the Ebola virus infection in 2014 [32] and cases of monkeypox in 2018 [33], both scenarios occurred in the UK. Contact tracking is a profoundly efficient and reliable strategy with adequate assets. The key benefit is that possible infected people can be detected before severe complications arise. If the process occurred in a short section, it could prevent the spread of the secondary cases. Contact tracing has demonstrated highly effective in treating viral infections in which the specific of contact is relatively simple. In contrast, the disease is frequently asymptomatic, and the propagation period- scales remain slow [34].
By comparison, contact tracking for new invading infections has received less systematic due to high ambiguity about the structure for social contact [35, 36]. The modeling works often concentrated on measuring the pre-symptomatic and pre-tracking disease’s significance but typically oriented on the numerical proportions of contact networks [37, 38]. We use expensive social network data from the UK to model spread ,traceability and to detect consequences for new microbes by using metrics compared to the COVID-19 in contact tracking [39, 30, 44].
Past modeling work analyzed the use of contact tracing in several infectious diseases, mainly smallpox [40] and STDs [41]. Contact tracing is tied closely to population interaction networks, including sexual partnership networks for STDs. Infection transmission usually occurs through interpersonal connections, and these known links also enable tracking of the development of infection [42]. They defined a mixing network to allow disease transmission between the number of individuals and link among the individuals, which is called a sexual mixing network. Here the author used a mathematical model, which is a single step and iterative contact-tracing schemes. This model analyses these practices capacity to locate primary groups and the sensitivity of the involvement to tracing time [43].
4 Materials And Methodology
4.1 Contact Tracing
Identifying highly infectious interactions has become a massive part of many prominent disease control strategies, ranging from early new infections to chronic sexually transmitted infections. Figure 3 explains contact tracing conditions for that person to be isolated, infected, and treatment to be provided. The contact tracing concept prevents the transmission of COVID-19 by the contacts disease-ridden and controls the COVID-19 epidemic [47]. This method takes a long delay to identify the transmission person, so a quick isolation process prevents the spreading of COVID-19.
To achieve the preventing transmission by contact tracing and isolation, a superior quantity of contacts, thus contact tracing using KNN method, is proposed in this paper.
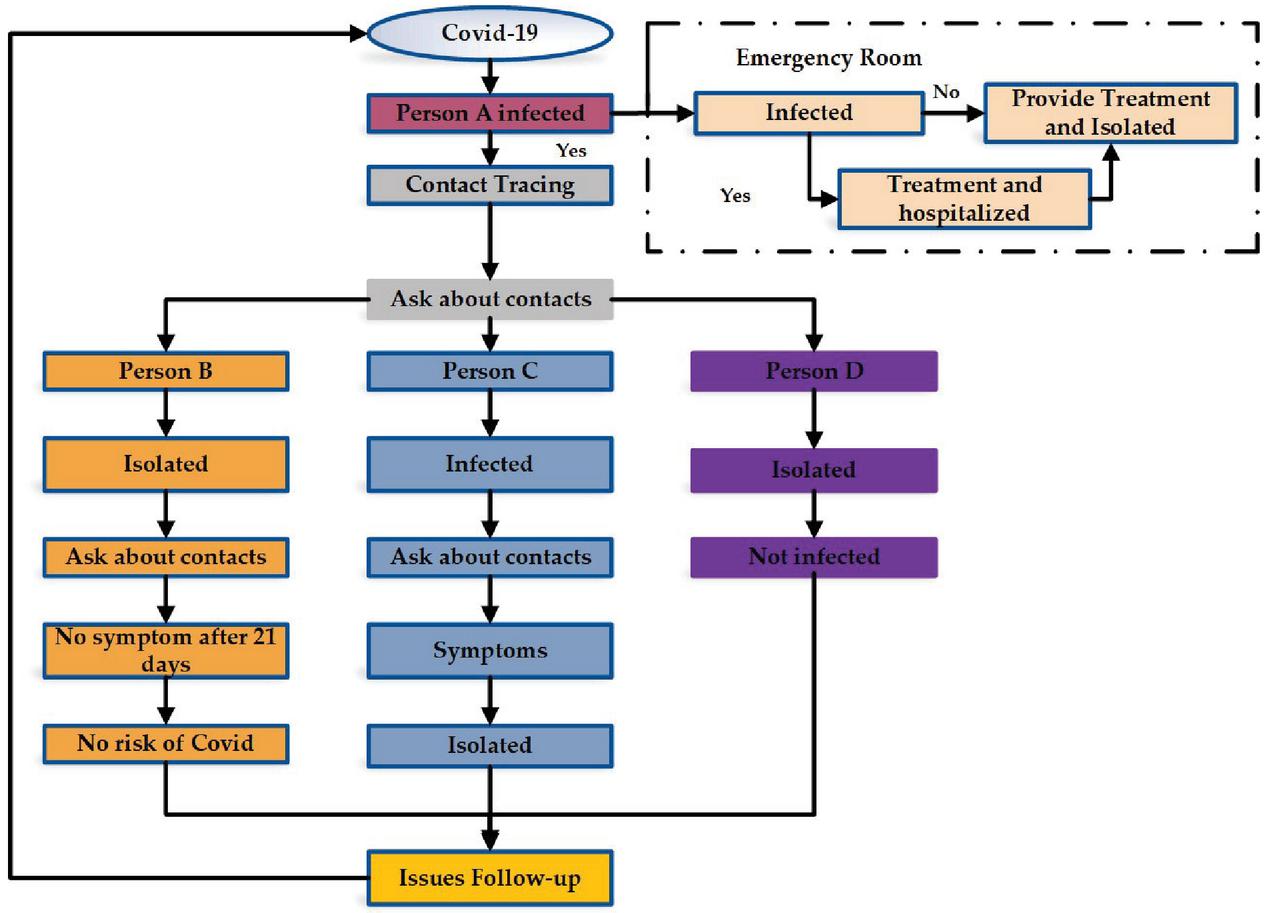
Figure 3 Simulated process of contact tracing of infected person COVID-19 [47].
4.2 Contact Tracing Using KNN For COVID-19
The data is reviewed on epidemiological analysis and medical records, respectively, from WHO, as described in Table 1. Infection carriers have been tested for clinical and group interactions. Because of the very high simplicity and precision, the KNN or K-Neighbors has one of the industry’s most standard classification algorithms. KNN is a modest algorithm that stores all essential data and categorizes new data based on a measure of similarity (e.g., distance functions) [45].
K-NN represents a number of nearest neighbours. It is a crucial factor in finding the closed contacts of the COVID-19 affected person. k is typically an odd number when the number of classes is 2. If k 1 is used, the algorithm is recognized as the nearest neighbour algorithm.
k-nearest neighbour classifier examines the training samples that are nearby to the unidentified trial. Nearness, it is generally expressions of distance from Euclidean. In this study, KNN is implemented using Euclidean distance to find the nearest neighbour based on the mathematical equation. X(x, x…x) and Y (y, y…y) are the two-point among Euclidean.
| (1) |
KNN classifier’s performance and precision predicate K selection and the distance metric applied in the COVID dataset [46]. In principle, the large K value is selected for smarter classification outcomes for the large sample size. Larger K provides more limits, better for generalization.
Table 1 Parameters from WHO dataset used in this study
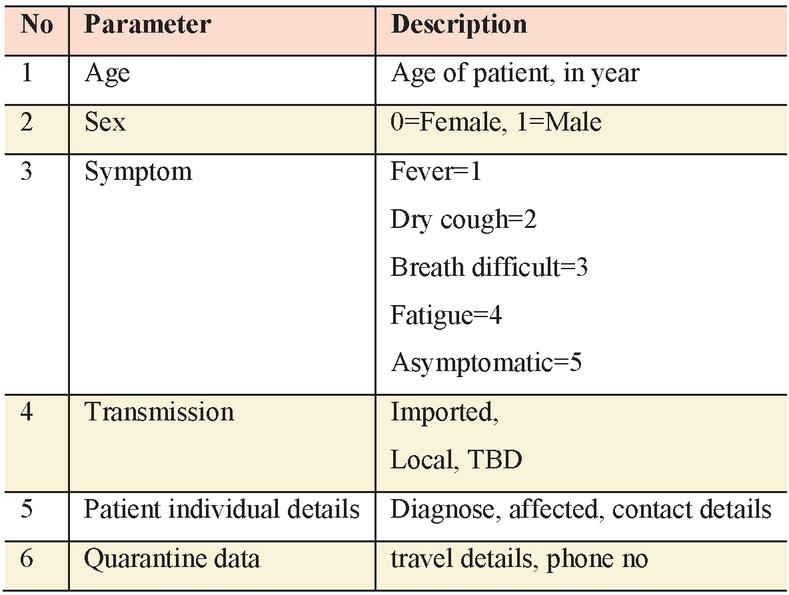 |
The above parameter is the outcome of the diagnosis and is the product of the estimation that a patient is stable (0) or has COVID-19 disease (1) [46]. The transmission of the COVID virus will be decreased by using the proposed method is described in Figure 4.
4.3 Processing of Contact Tracing Using KNN
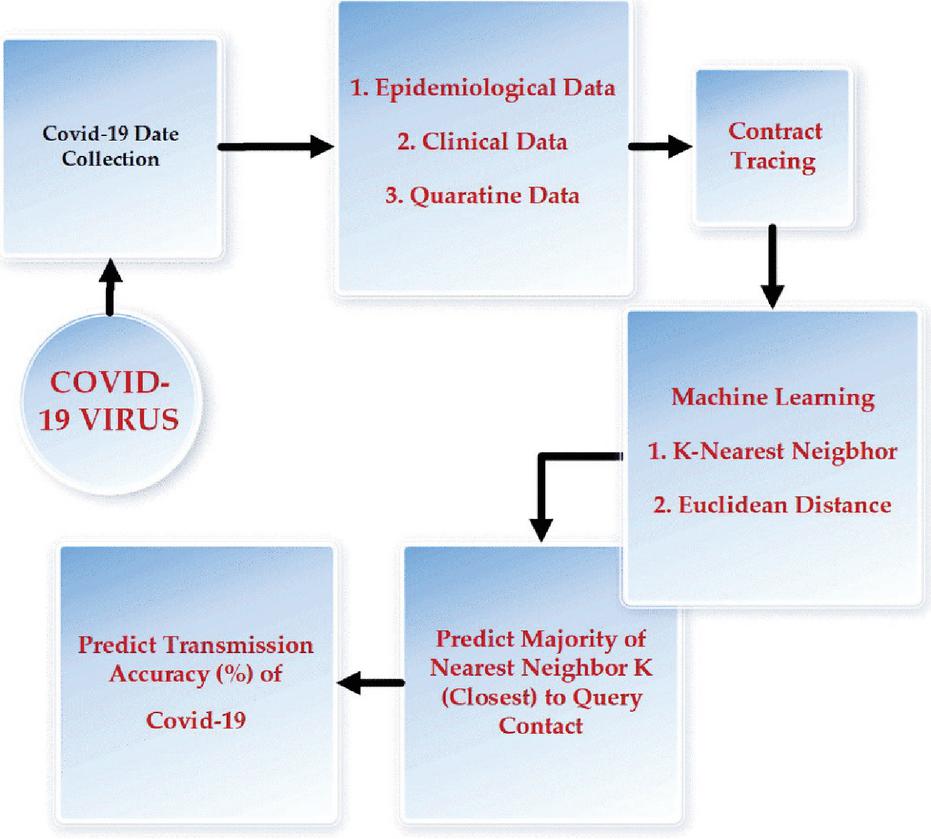
Figure 4 Proposed contact tracing using KNN-an overview diagram.
5 Experimental Results
Our experimental results show that the contact tracing using KNN has controlled the transmission of spreading COVID-19 at the initial stage and gives an average accuracy of 85% as shown in Figure 5. In contrast, the contact tracing method gives an accuracy of 77% by contact tracing probability [46, 47]. The accuracy of the contact details of the affected person of COVID-19 can be easily predictable using the proposed methodology, elaborated in the materials and methodology section.
We discover the most frequent collection of parameters well-versed by the newest data on the spread of COVID-19. The comparison result is shown in Figure 6, where the most frequent feature is voted and labeled in COVID-19. Using KNN is applied to the proposed method, general contact tracing to find the comparison result accuracy for the features.
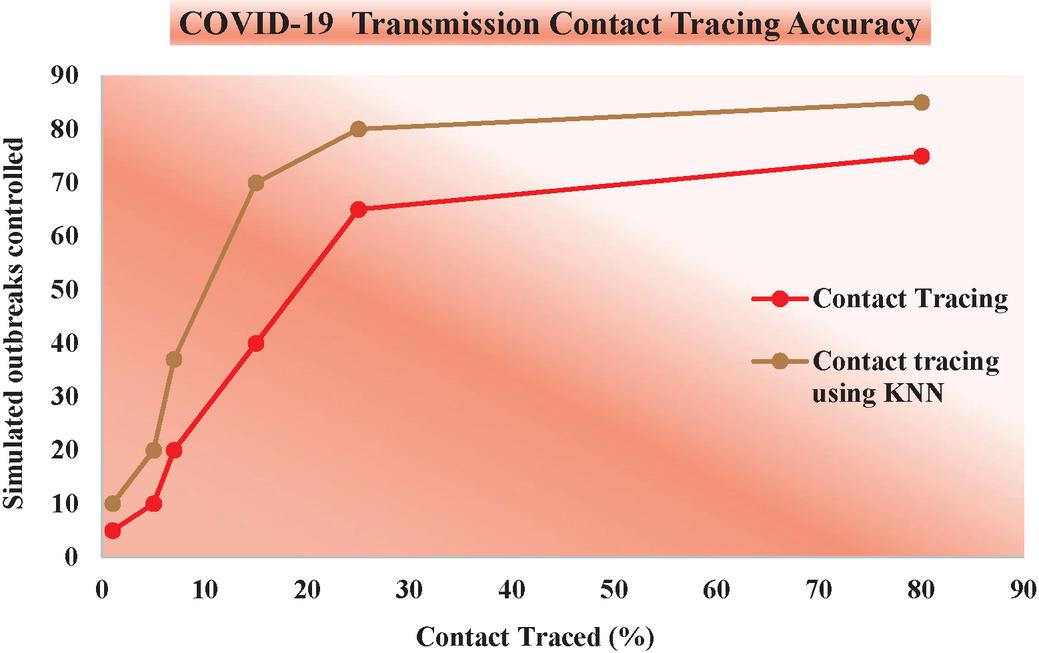
Figure 5 COVID-19 transmission contact tracing accuracy.
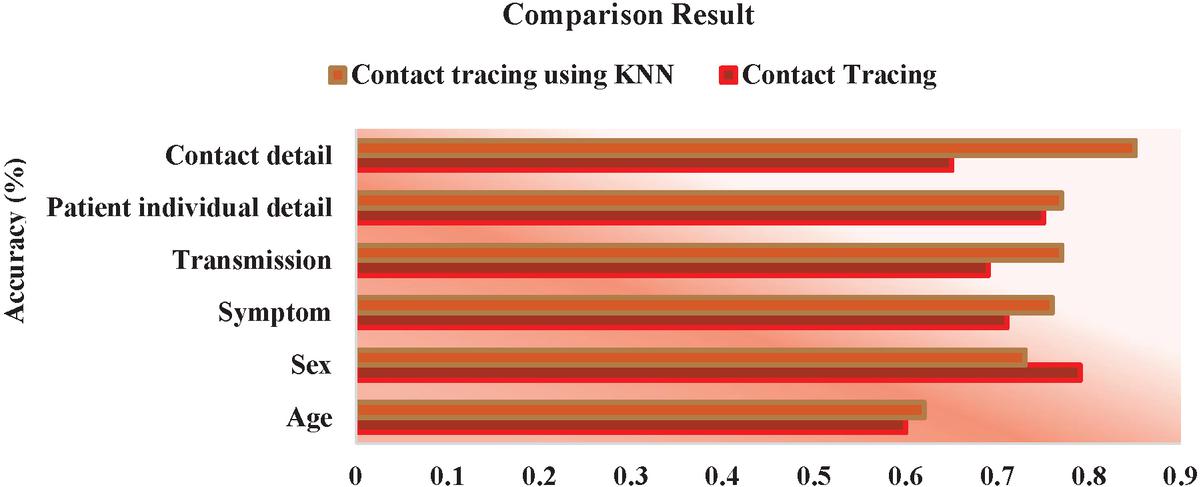
Figure 6 Comparison result of contact tracing and proposed contact tracing with KNN.
6 Conclusion
This paper deliberates the data classification of Covid-19 and the selection of features. The proposed work creates the effectiveness of diagnosing Covid-19 disease close contact details and decreasing the transmission. A combined method of contact tracing and KNN used to optimize the feature selection, and the KNN algorithm was used to classify and diagnose the affected person’s contact details of COVID-19. The suggested algorithm aimed to present a better classification with fewer data features and assess accuracy effectiveness. Data on this test is obtained from the World Health Organization (WHO). Similar analyses using contact tracing have already been used to analyze the closed contact, but its drawbacks in a long delay in finding transmission and control outbreaks. Our analysis expands this work using KNN to find the similarly affected persons in neighbouring proximity in a short period and improves accuracy. In the future, machine learning algorithms aid massively in data classification of medical data, and future interventions would be required to achieve control epidemic.
References
[1] Mannan, N., & Akram, A. (2020). Variation of Clinical Features of Covid19 Patients. Bangladesh Journal of Infectious Diseases, S54–S57.
[2] “World Health Organisation”, Coronavirus press conference, released on February 11 2020.
[3] World Health Organization. (2005). Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV).
[4] World Health Organization. (2020). Coronavirus disease 2019 (COVID-19): situation report, 72.
[5] Perlman, S., & Netland, J. (2009). “Coronaviruses post-SARS: update on replication and pathogenesis. nature reviews microbiology”, 7(6), 439–450.
[6] Al-Sharif, E., Strianese, D., AlMadhi, N. H., D’Aponte, A., dell’Omo, R., Di Benedetto, R., & Costagliola, C. (2020). Ocular tropism of coronavirus (CoVs): a comparison of the interaction between the animal-to-human transmitted coronaviruses (SARS-CoV-1, SARS-CoV-2, MERS-CoV, CoV-229E, NL63, OC43, HKU1) and the eye. International ophthalmology, 1–14.
[7] World Health Organization. Q&A on coronaviruses (COVID-19). March 9 2020.
[8] Chen, N., Zhou, M., Dong, X., Qu, J., Gong, F., Han, Y., & Yu, T. (2020). Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. The Lancet, 395(10223), 507–513.
[9] Wang, D., Hu, B., Hu, C., Zhu, F., Liu, X., Zhang, J., & Zhao, Y. (2020). Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. Jama, 323(11), 1061–1069.
[10] Centers for Disease Control. (2020). Interim clinical guidelines for the management of patients with confirmed coronavirus disease (COVID-19).
[11] Lauer, S. A., Grantz, K. H., Bi, Q., Jones, F. K., Zheng, Q., Meredith, H. R., & Lessler, J. (2020). The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: estimation and application. Annals of internal medicine.
[12] Kumar, S., Maheshwari, V., Prabhu, J., Prasanna, M., Jayalakshmi, P., Suganya, P., …& Jothikumar, R. (2020). Social economic impact of COVID-19 outbreak in India. International Journal of Pervasive Computing and Communications, 16(4):309–319
[13] Lai, C. C., Shih, T. P., Ko, W. C., Tang, H. J., & Hsueh, P. R. (2020). Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): the epidemic and the challenges. International journal of antimicrobial agents, 105924.
[14] Priya, K. B., Rajendran, P., Kumar, S., Prabhu, J., Rajendran, S., Kumar, P. J., …& Jothikumar, R. (2020). Pediatric and geriatric immunity network mobile computational model for COVID-19. International Journal of Pervasive Computing and Communications. 16(4):321–330.
[15] Wilder-Smith, A., & Freedman, D. O. (2020). Isolation, quarantine, social distancing and community containment: a pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. Journal of travel medicine, 27(2), taaa020.
[16] Grenfell, R., & Drew, T. (2020). Here’s Why It’s Taking So Long to Develop a Vaccine for the New Coronavirus. Science Alert. Archived from the original on, 28.
[17] Venkatasen, M., Mathivanan, S. K., Jayagopal, P., Mani, P., Rajendran, S., Subramaniam, U., …& Somanathan, M. S. (2020). Forecasting of the SARS-CoV-2 epidemic in India using SIR model, flatten curve and herd immunity. Journal of ambient intelligence and humanized computing, 1–9
[18] Wiles, S. (2020). After ‘Flatten the Curve’, we must now ‘Stop the Spread’. Here’s what that means. The Spinoff.
[19] Huynh, T. D. (2020). The more I fear about COVID-19, the more I wear medical masks: A survey on risk perception and medical masks use. medRxiv.
[20] Safety, E. (2016). And Prevention of Coronavirus Disease 2019 (COVID-19) in Nursing Homes (Revised 03/13/20).
[21] World Health Organization (WHO). Shortage of personal protective equipment endangering health workers worldwide: WHO; 2020 [March 11, 2020].
[22] Coia, J. E., Ritchie, L., Adisesh, A., Booth, C. M., Bradley, C., Bunyan, D., …& Phin, N. (2013). Guidance on the use of respiratory and facial protection equipment. Journal of Hospital Infection, 85(3), 170–182.
[23] Shereen, M. A., Khan, S., Kazmi, A., Bashir, N., & Siddique, R. (2020). COVID-19 infection: origin, transmission, and characteristics of human coronaviruses. Journal of Advanced Research.
[24] https://www.mbc.news/n/2020/04/contact-tracing-swiss-app-developer-says-what-is-important.html
[25] Biggerstaff, M., Cauchemez, S., Reed, C., Gambhir, M., & Finelli, L. (2014). Estimates of the reproduction number for the seasonal, pandemic, and zoonotic influenza: a systematic review of the literature. BMC infectious diseases, 14(1), 480.
[26] WHO Ebola Response Team. (2014). Ebola virus disease in West Africa—the first 9 months of the epidemic and forward projections. New England Journal of Medicine, 371(16), 1481–1495.
[27] Althaus, C. L. (2014). Estimating the reproduction number of Ebola virus (EBOV) during the 2014 outbreak in West Africa. PLoS currents, 6.
[28] Mills, C. E., Robins, J. M., & Lipsitch, M. (2004). Transmissibility of 1918 pandemic influenza. Nature, 432(7019), 904–906.
[29] Kaner, J., & Schaack, S. (2016). Understanding Ebola: the 2014 epidemic. Globalization and health, 12(1), 53.
[30] Bootsma, M. C., & Ferguson, N. M. (2007). The effect of public health measures on the 1918 influenza pandemic in US cities. Proceedings of the National Academy of Sciences, 104(18), 7588–7593.
[31] Hébert-Dufresne, L., Althouse, B. M., Scarpino, S. V., & Allard, A. (2020). Beyond : the importance of contact tracing when predicting epidemics. arXiv preprint arXiv:2002.04004.
[32] McLean, E., Pebody, R. G., Campbell, C., Chamberland, M., Hawkins, C., Nguyen-Van-Tam, J. S., …& Maguire, H. (2010). Pandemic (H1N1) 2009 influenza in the UK: clinical and epidemiological findings from the first few hundred (FF100) cases. Epidemiology & Infection, 138(11), 1531–1541.
[33] Crook, P., Smith-Palmer, A., Maguire, H., McCarthy, N., Kirkbride, H., Court, B., …& Oliver, I. (2017). Lack of Secondary Transmission of Ebola Virus from Healthcare Worker to 238 Contacts, United Kingdom, December 2014. Emerging infectious diseases, 23(12), 2081.
[34] Vaughan, A., Aarons, E., Astbury, J., Balasegaram, S., Beadsworth, M., Beck, C. R., & Harper, N. (2018). Two cases of monkeypox imported to the United Kingdom, September 2018. Eurosurveillance, 23(38).
[35] Hoang, T., Coletti, P., Melegaro, A., Wallinga, J., Grijalva, C. G., Edmunds, J. W., …& Hens, N. (2019). A systematic review of social contact surveys to inform transmission models of close-contact infections. Epidemiology, 30(5), 723–736.
[36] Ahmed, F., Zviedrite, N., & Uzicanin, A. (2018). Effectiveness of workplace social distancing measures in reducing influenza transmission: a systematic review. BMC public health, 18(1), 518.
[37] Hoang, T., Coletti, P., Melegaro, A., Wallinga, J., Grijalva, C. G., Edmunds, J. W., …& Hens, N. (2019). A systematic review of social contact surveys to inform transmission models of close-contact infections. Epidemiology, 30(5), 723–736.
[38] Fraser, C., Riley, S., Anderson, R. M., & Ferguson, N. M. (2004). Factors that make an infectious disease outbreak controllable. Proceedings of the National Academy of Sciences, 101(16), 6146–6151.
[39] Kwok, K. O., Tang, A., Wei, V. W., Park, W. H., Yeoh, E. K., & Riley, S. (2019). Epidemic Models of Contact Tracing: Systematic Review of Transmission Studies of Severe Acute Respiratory Syndrome and Middle East Respiratory Syndrome. Computational and structural biotechnology journal.
[40] Fraser C, et al. Factors that make an infectious disease outbreak controllable. Proceedings of the National Academy of Sciences USA 2004; 101: 6146–6151.
[41] Kretzschmar M, van Duynhoven YTHP, Severijnen AJ. Modeling prevention strategies for gonorrhea and chlamydia using stochastic network simulations. American Journal of Epidemiology 1996; 144: 306–317.
[42] Jolly AM, Wylie JL. Gonorrhea and chlamydia core groups and sexual networks in Manitoba. Sexually Transmitted Infection 2002; 78: i145–51.
[43] KTD. Eames, Contact tracing strategies in heterogeneous populations.Epidemiol Infect.2007, Apr, 135(3), pp. 443–454.
[44] Read, J. M., Bridgen, J. R., Cummings, D. A., Ho, A., & Jewell, C. P. (2020). Novel coronavirus 2019-nCoV: early estimation of epidemiological parameters and epidemic predictions. MedRxiv
[45] Li, Q., Guan, X., Wu, P., Wang, X., Zhou, L., Tong, Y., & Xing, X. (2020). Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. New England Journal of Medicine.
[46] Zhang, S., Li, X., Zong, M., Zhu, X., & Cheng, D. (2017). Learning k for kNN classification. ACM Transactions on Intelligent Systems and Technology (TIST), 8(3), 1–19.
[47] https://www.who.int/gho/database/en/covid-19
[48] Hellewell, J., Abbott, S., Gimma, A., Bosse, N. I., Jarvis, C. I., Russell, T. W., & Flasche, S. (2020). Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. The Lancet Global Health.
Biographies

Maheshwari Venkatasen has completed M.S (By Research) in Computer Science from the Vellore institute of technology. Presently she is pursuing a Ph.D. at Vellore Institute of Technology, Vellore, Tamil Nadu. She has published many papers in reputed journals—her current area of research interest in Blockchain security, Software Engineering, Security testing, Machine Learning.

Sandeep Kumar Mathivanan received an M.S degree in Software engineering from the Vellore Institute of Technology (VIT), Vellore, India, in 2016, and the M.Tech (By research) degree from VIT in 2020, where he is currently pursuing the Ph.D. degree with the School of Information Technology and Engineering. His current research interests include Machine learning, Big data analytics, Recommender systems, Virtualization, Blockchain. He is the author/co-author of papers in International Journals, Conferences, and book chapters.

Prasanna Mani has completed his M.S. in Computer Science from Anna University. He received his doctorate in Software Engineering from Anna University. Presently he is working as Associate Professor in Vellore Institute of Technology Vellore (Deemed to be University), Vellore, Tamil Nadu. He has published nearly 30 papers in various national and international journals. He is guiding Research scholars in the area of Software testing and is an eminent reviewer of various international journals. He also authored a book for cracking interview questions of C programming. His area of interest includes Software Engineering, Software Testing, and the Internet of Things.

Prabhu Jayagopal received the bachelor’s degree in Information Technology from the University of Madras Under Vellore Engineering College, Vellore, India, in 2004, the master’s degree in Computer science and engineering from Sathyabama University, Chennai, India, in 2007, and the Ph.D. degree in Computer Science and Engineering from Sathyabama University, Chennai, India in 2015. He worked as an Assistant Professor in various Engineering colleges for more than 14 years. Now he is working as an Associate Professor in the School of Information Technology and Engineering, Vellore Institute of Technology, Vellore, from 2009 to date. He has published in National, International journals and conferences. He is also involved in collaborative research projects with various national and international level organizations and research institutions. His research interests are software testing, Machine Learning, Deep Learning, and Big data.

Thanapal P received his B.E degree in Computer Science and Engineering from Madurai Kamaraj University, Madurai India in 1998, M.E degree in Computer Science and Engineering from Anna University Chennai, India, in 2005, and a Ph.D. degree from Vellore Institute of Technology University Vellore, India. He has published more than 30 research papers in reputed international journals and conferences. His main research interests include cloud computing, mobile cloud computing, wireless network, and IoT.

Manivannan Sorakaya Somanathan is working as Associate Professor in the Information Technology Department at VIT University, Vellore. He has completed a Ph.D. in the domain of network and information security in the School of Information Technology and Engineering, VIT University, Vellore. Also, he has B.E and M.E degrees in the area of Computer Science and Engineering at the University of Madras and Anna University, Chennai, respectively. He has 15 years of experience and standard publications in reputed journals.
Upendra Babu K received his bachelor’s degree in Computer science and Engineering from Karnataka University, Dharwad, Karnataka, under Rural Engineering college, Hulkoti, Gadag, Karnataka in 2000, and master’s degree also in Computer science and Engineering from Dr. M.G.R. University, Chennai, India, in 2011, and is pursuing his Ph.D. degree in Computer Science and Engineering at Manonmaniam Sundaranar University, Tirunelveli, India. He has over 17 years of experience as an Assistant Professor in various Engineering colleges. He is currently pursuing a Ph.D. He has had several articles published in national and international journals. He also participates in collaborative research projects with several national and international organizations and research institutions. Data Mining, Machine Learning, Deep Learning, Big Data, Artificial Intelligence, and Image Processing are among his research interests.

Elangovan D is working as an Associate Professor in Computer Science and Engineering Department at Panimalar Engineering College, Chennai. He has teaching experience of more than two decades. He has published many papers in international journals and conferences. He has filed few patents also. He actively took part in conducting conferences, FDPs, and seminars.
Journal of Mobile Multimedia, Vol. 17_4, 789–808.
doi: 10.13052/jmm1550-4646.17415
© 2021 River Publishers