Intelligent Personal Health Monitoring and Guidance Using Long Short-Term Memory
S. Velliangiri1, V. Anbarasu2, P. Karthikeyan3,* and S. P. Anandaraj4
1B V Raju Institute of Technology, Narasapur, Telangana, India
2Department of Networking and Communications, School of Computing, SRM Institute of Science and Technology, Katankulathur, Chennai, India
3Computer Science and Engineering, Jain (Deemed-to-be University), Bangalore
4CSE in Presidency University, Bangalore, India
E-mail: nrmkarthi@gmail.com
*Corresponding Author
Received 16 June 2021; Accepted 21 August 2021; Publication 29 October 2021
Abstract
Rapid improvements in information technology have made everything in this world contemporary. The mobile phone plays a vital role in the day to day activities. Many mobile applications are developed by using deep learning models to give health guidance to people. We proposed intelligent personal health monitoring and guidance (IPHMG) using long short-term memory to assess the users’ overall health status to solve the mobile application performance problem. The main objective of the research work is to minimize the delay time of the user’s request and improve the accuracy of health predictions. The proposed system calculates scores using the IPHMG score model to find the health conditions of the users. IPHMG score model uses different time-series data to calculate scores such as environment data, body signal data, parent report data, emotion, and health report. Additionally, an Android application is a module that is designed for mobile users to feed their health data and check their health status. The proposed system was implemented. Results show that the proposed method provides better uploading time, processing time, and the user downloading time than simple RNN and ANN methods.
Keywords: Artificial neural network, recurrent neural network, LSTM, Android application, IPHMG.
1 Introduction
The world health organization stated that many people died because of non-communicable diseases like diabetes, Alzheimer’s, cancer, osteoporosis, chronic lung disease, stroke, and heart diseases. These diseases are caused because of the bothersome lifestyles of a person. The people are not understanding or not measuring their health status because of this many death happened. The world health organization proposes a manual for people, including lifestyles, including smoking, alcohol misuse, nonappearance of movement, outlandish salt statement, etc. Smartphone plays an essential role in individual life. Advancements in the portable programming application are of potential advantages to general wellbeing since versatile stages become easier to understand, computationally incredible, and reasonable. We need to develop simple Android applications that help patients find out and treat their diseases. To predict humans’ diseases and avoid death, we can use the mobile phone to capture our daily generated data in mobile, parent data, health reports, and emotion and passed to the system, giving detailed descriptions [1, 2].
Recent many deep learning methods have been proposed to predict the psychical disease of the human. However, the proposed system has the following limitations. The data set used in the model is small because of mobile phone limitations. This data is inadequate to screen the client’s long term status thoroughly. Simple operation is supported like monitoring the health status of users and give warning to the users. The system should provide a detailed report to the users about their health conditions. In order to solve the problem mentioned above, we proposed comprehensive intelligent personal health monitoring and guidance (IPHMG) using long short-term memory. The IPHMG is principally designed to detect, diagnose, and provide medication suggestions for the day-to-day ailments of humans. We have developed an Android application that avoids the side effects of taking medicines without a doctor’s suggestion [3, 4]. Users can rightly find out their diseases from the specific symptoms given in this android application. Its dosage is added into the database from which the users can retrieve the medication details. The mobile application also lists the conditions of medical emergencies where the situations are proved to be adverse and need doctor consultation for surgical procedures to be followed immediately. Moreover, in those cases too, users can get the antibiotic combination used after the surgery in this app. Thus the patient can also cross-check with the prescriptions given by the doctors for finding out the negligence [5, 6]. RNNs cannot work with more extended schedules and hold long term conditions, triggering them to experience the ill effects of “short-lived memory”. IPHMG uses long short-term memory (LSTM) to process and predict the disease of humans to avoid death. LSTM presents something many refer to as a memory cell. LSTM has different memory cells to store the information and accurate predictions [7, 8].
The proposed system gives an interface to the Android application, which takes input from mobile users and gives the health status of mobile users. Earlier days, if the patient needs to predict his health status, he has gone to the hospital, and examination is performed on him, conduct test. After that, the doctor will use the patient report, and then he will predict the status of the users. The manual process consumes the time and labour of the patient, and at times the user might have had a minor complication, which would have required some tiny tablets [9]. In the modern era lot of mobile applications have also been developed for assessing health status. The proposed application is of enormous advantage to the patient. It provides all the details necessary for the users to self-medicate at its best, professional level and saves their time, labour, costs, and lives [10].
The significant contribution of the paper is outlined as follows.
1. Designed intelligent personal health monitoring and guidance using long short-term memory and tested in a real-time environment.
2. We have developed a mobile interface to interact with the proposed system and test the health conditions of the mobile users.
3. We have compared performances of proposed system LSTM with simple RNN and ANN deep learning method.
The rest of the paper is organized as follows: Section 2 discusses the existing deep learning method used in health care for predicting diseases. Section 3 deals with the proposed model and algorithm. We have discussed results discussion in Section 4, and Section 5 consists of the conclusion and future work.
2 Related Work
Pasupathi and Kalavakonda et al. proposed evidence-based medicine and big data analytics to improve the quality of healthful treatment. The proposed system is analyzed, and it performs well at the personal computer level. It is not giving good performances in the mobile application [11]. Series and Report proposed a clinical decision support system. It takes clinical practice guidelines and uses an automatic converter to generate CPG rules. Here any questions from the physicians can be obtained from the knowledge base using the inference engine. The proposed framework is coordinated in the doctor’s work process. It will improve patient consideration by giving proof at the right time and spot. The system contains four modules to deal with every perspective in essential clinical leadership and rules the board [12].
Abouzahra et al. designed an electronic health record (EHR) based data integration model. The proposed model provides a clinical remedy for inflammatory bowel disease. It fragmented the entire dataset of the patient from EHR systems. The fragmented data are used by the proposed method aggregate information from different quiet related frameworks. In the long run, this would fabricate an archive of patient information that clinicians can utilise genuinely [13]. Chen et al. proposed an intelligent personal health advisor (SPHA) based on deep analytics to check users’ health status and acknowledge the perception of clients’ close to home estimations and social qualities to direct them to have more advantageous ways of life. SPHA takes three different types of users to input: mental status, individual worth, and social worth. The outcomes have demonstrated that the SPHA gives good health status to the users with less delay time [14]. Sakr and Elgammal reported that cloud computing, big data, and IoT contribute towards improving the productivity and viability of medicinal services administrations. The proposed model has benefits in keen medicinal services systems, Smart Health, which reveals difficulties and fills in the recognized holes. The system additionally goes about as a guide for future research endeavours in the zone of massive information investigation in shrewd social insurance applications [15].
Vijayakumar et al. presented a framework to separate the mosquito-borne infections and analyze the client whether he/she is influenced by such disease or not. The proposed model uses the K-nearest neighbour machine learning algorithm to classify mosquito-borne infections based on signs/manifestations [16]. Bhatia and Sood discussed an intelligent framework for workouts in the gymnasium social insurance forecast model utilizing cloud computing IoT Technology. The proposed model uses an artificial neural network to predict the status of the health condition of users. Results showed that the proposed model could enrol better in examination than the traditional machine learning model [17].
Hii et al. discussed that healthcare applications use wireless sensor networks (WSN) for health data exchange. Remotely transmitting the ECG signal in a WSN can diminish the problem of conventional wired ECG machines, give a perfect and stable ECG sign without a doubt time heart mood examination. Other than moving medicinal services from clinical-driven to quiet driven, this thought would likewise move the social insurance from treatment to aversion. The initial discovery of illnesses may give a recuperation opportunity to the patient [18].
Khovrichev et al. developed clinical remote monitoring systems. The proposed approach consolidates the medicinal and research frameworks to illuminate information readiness for further demonstrating procedures without impediments on conventions [19]. Yong et al. proposed an IoT based intelligent fitness system for wellness clubs. In the interim, they attempt to utilize artificial intelligence innovation in the framework to execute the work. It is essential to concentrate on the blend of wellbeing and human-made reasoning. In any case, there are a few issues that need further investigates, for example, the exact connections between pulse and wellbeing [20].
Yang et al. exhibited another pulse identification technique that consolidated savvy terminal and edge processing to understand a human services IoT framework. In this preliminary analysis information, when the SNR is lower to 8.9 dB, it very well may be caused to expand the mistake pace of pulse estimation and got the wrong pulse since its pulse sign is excessively low [21].
About et al. suggested fetal health status prediction based on maternal clinical history using machine learning techniques. Dataset is used in this model is small, and AI approach, the forecast of a specific component can be acquired. This capacity can help specialists avoid potential risks or break down an issue more in-depth [22]. Yuksel et al. proposed a bidirectional LSTM Recurrent Neural Network structure to identify understudies’ disarray. The exactness accomplished by the proposed model is higher than other AI approaches, including a solitary layer RNNLSTM model, and accomplishes the best in class result. The design of the Bidirectional LSTM model exploits time-arrangement highlights and improves execution [23]. Smith et al. designed a mobile application for behavioural studies. The mobile application gives specialists a cutting-edge innovation stage to contemplate human conduct concerning liquor utilization and hazard taking propensities. The mobile application likewise exhibited a proof-based way to incorporate proper conduct and specialized regions [24]. Based on this inference, we proposed an intelligent personal health monitoring and guidance system using the LSTM machine learning method.
3 Intelligent Personal Health MONITORING and Guidance System
Intelligent personal health monitoring and guidance using long short-term memory use a simple Android application designated to provide suggestions regarding emotion detection, psychological status, user behaviour statuses, and potential diseases. The application gives the details in the hierarchy as follows. First, users have created an account, and he has validated his account using an Android phone. Once it is over, he has provided input data such as social skills, health-related information, environment information, behaviour information, and parent history information. Besides, the IPHMG is intended to give the IPHMG-Score to clients. IPHMG uses simple Android applications designed to detect, diagnose, and provide medication-related suggestions for the day-to-day ailments of humans. It avoids the side effects that occur to humans on taking medicines without a doctor’s opinion. Users can rightly find out their diseases from the specific symptoms given in this app. The doctor suggested medicines for every ailment. Its dosage is added into the database from which the users can retrieve the medication details. Further, the app also lists the conditions of medical emergencies where the situations are proved to be adverse and need doctor consultation for surgical procedures to be followed immediately.
Moreover, in those cases too, users can get the antibiotic combination used after the surgery in this app. Thus any malpractices or wrong medication done by the doctors can be found out quickly, making users self-aware. As mobile technology continues to evolve and shape human interaction with technology, Human-Centered Design (HCD) methods adapt to the capabilities of technology and the needs of mobile application development. This study aims to highlight emerging practices and their implications for mobile application development. The main drawback is that none of the papers explained above gives a complete medical solution. They are particular for specific symptoms or diseases. The disadvantages are mainly seen when either the patient lacks the motivation or does not have sufficient education on interpreting the results to make adequate home testing equipment. It also wastes the time of the patient. The general design of intelligent personal health monitoring and guidance using LSTM has appeared in Figure 1.
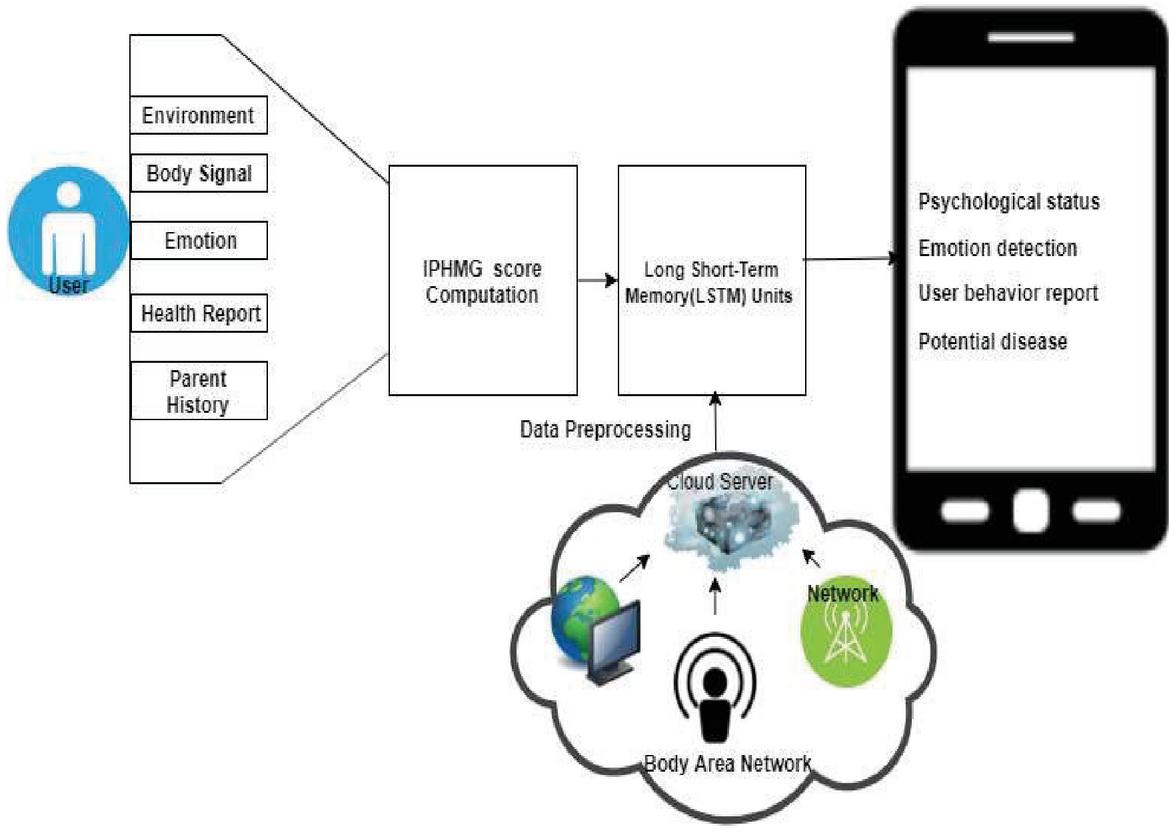
Figure 1 Intelligent personal health monitoring and guidance using LSTM.
Each client has an individual IPHMG Score. Each “bloom” represents a client who has his/her very own IPHMG-Score framework. Different systems administration and correspondence frameworks gather the information, psychological structures, the Internet of Things (IoT), body region systems, mechanical technology, etc. The level incorporates three segments: information grouping (i.e., the characterization on measurements information, time arrangement information, and content information), information preprocessing, which includes information decrease, information change, what is more, information cleaning, and information examination, in light of AI, deep learning, and intellectual model. The “petal” level mirrors the aftereffects of physiological or mental examination of the client, which incorporates feeling identification, conduct examination, weariness location, physiological status checking, passionate consideration, potential illness investigation, social effect examination, subjective setting examination, etc. The “stamen and pistil” level speaks to the goal of the IPHMG score framework. Figure 2 shows the IPHMG score framework.
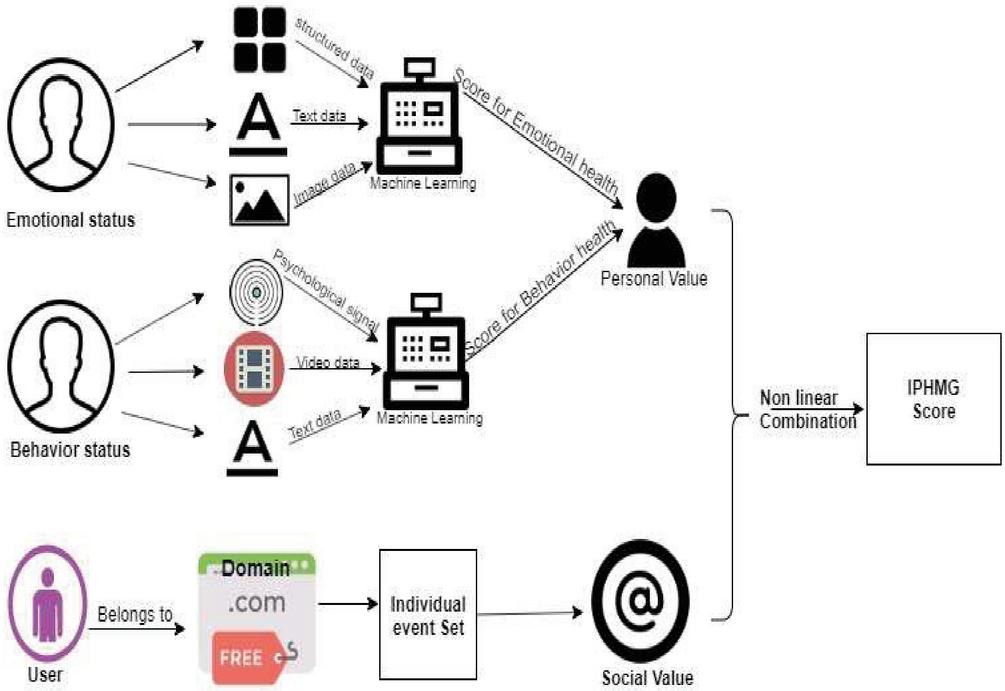
Figure 2 IPHMG score framework.
Long Short-Term Memory Units (LSTMs)
LSTM can be used to process and classify the time series of data by storing the information for an extended period. LSTM contains cell, input gate, an output gate, and forgets gate. LSTM uses cells to store data and gate manipulate the information that is present in the cell. There are three different types of gates used in LSTM, such as the input gate, output gate, and forget gate. Forget gate remove the irrelevant information in the cell and keep essential or relevant information in the cell. Forget gate use the sigmoid function to remove the unnecessary information in the cell and pairwise multiplication to retain important information in the cell. The sigmoid function takes the values zero to one. Zero means it will not remove any information, and one means it will remove the entire information. The cell at that point utilizes entryways to manage the data to be kept or disposed of at each time step before passing on the long haul and transient data to the following cell. These doors can be viewed as water channels. In a perfect world, the job of these doors should precisely expel any superfluous data, like how water channels keep polluting influences from going through. Simultaneously, just water and helpful supplements can go through these channels, much like how the doors clutch the valuable data. These entryways should be prepared to precisely channel what is useful and what is not. These doors are known as the Input Gate, the Forget Gate, and the Output Gate. There are numerous variations to the names of these doors; all things considered, the estimations and activities of these entryways are, for the most part, the equivalent.
Input Gate: The information entryway chooses what new data will be put away in the long term memory. Hence, it needs to sift through the data from these factors that are not helpful. Scientifically, this is accomplished utilizing two layers. The first layer can be viewed as the channel which chooses what data can go through it and what data to be disposed of in the state. To make this layer, we pass the short memory and current contribution to a sigmoid capacity. The sigmoid size will change the qualities somewhere between 0 and 1, with 0 demonstrating that the data is immaterial.
Forget Gate: The forget gate decide which information in the cell state has to forget. To get the overlook vector, the short memory and current information are gone through a sigmoid capacity, like the main layer in the Input Gate above, yet with various loads. The vector will comprise 0 s and 1 s and will be increased with the long deep memory to pick which parts of the long deep memory to retain.
Output Gate: Output gate will take the present info, the past momentary memory, and the recently figured long haul memory to create the new transient memory/concealed state, which will be given to the cell whenever step. The yield of the present time step can likewise be drawn from this concealed state. The yield from these two procedures will be increased to create the new present moment memory. The present moment and long haul memory delivered by these doors will, at that point, be extended to the following cell for the procedure to be rehashed. The yield of each time step can be gotten from the short memory, otherwise called the shrouded state. Figure 3 shows the internal working process of LSTM filters.
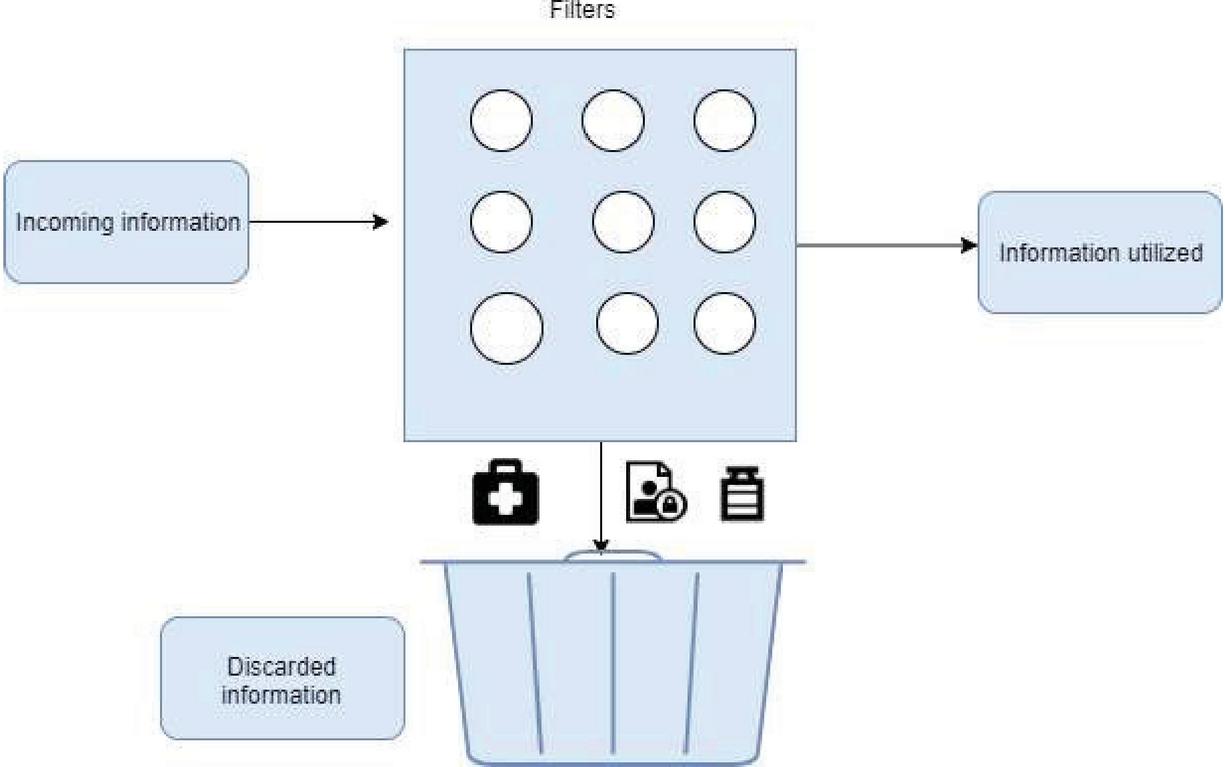
Figure 3 LSTM filters.
The LSTM process flow is presented in Figure 4, and the LSTM step by step process is described as follows.
1. First, the step in the LSTM is to decide which information has to keep and which data has been removed. The sigmoid layer does this function. It looks at ht-1 and xt, and outputs a number between 0 and 1 for each cell state Ct-1. ft vale is zero means complete cell value is removed, and one means wholly kept in the cell
| (1) |
2. The second step is to decide what information we are going to keep and the pairwise operation. This has two parts previous hidden state, and the current input state is combined, and it is given to the forget gate. Forget gate perform the pairwise operation and keep the vital information in the cell.
| (2) |
The layer creates a vector of new candidate values, C~t, that could be added to the state.
| (3) |
3. The third step is to merge these two to make an update to the state. It is at present to resuscitate the old cell state, Ct-1, into the new cell state Ct. the past advances as of late picked what to do, and we need to do it. We increase the old state by ft, disregarding the things we chose to overlook already. By that point, we consolidate itCt. This is the new up-and-comer respect, scaled by the entirety we wanted to resuscitate each state regard. Finally, we have to pick what we are going to yield. This yield will be set up on our cell state, yet it will be a disengaged change. In any case, we run a sigmoid layer that picks what parts of the cell state we will yield. At that point, we put the cell state through tanh (to drive the attributes to be some spot in the extent of 1 and 1) and add it by the yield of the sigmoid entrance, with the target that we yield the parts.
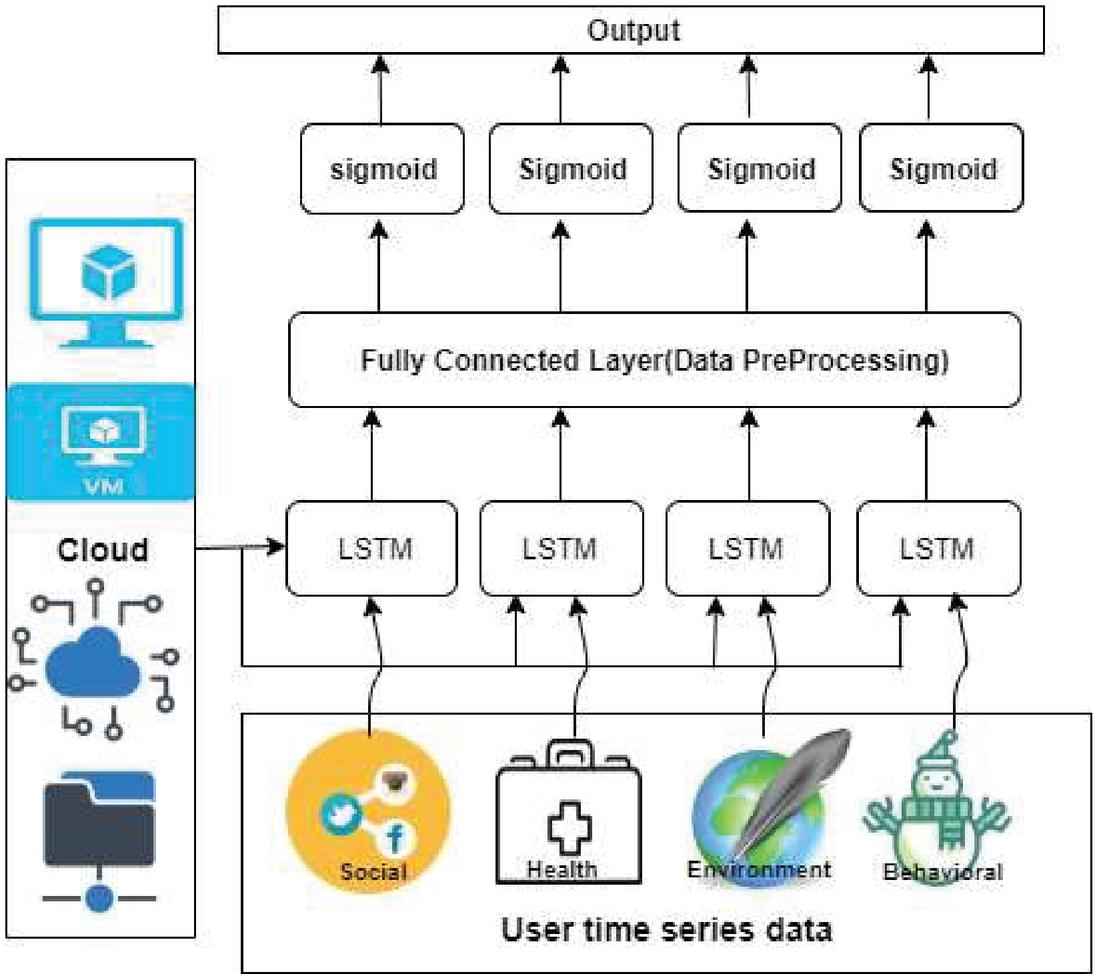
Figure 4 Long short-term memory units.
4 Results and Discussion
LSTM model designed and tested in an open nebula based virtual datacenter. Table 1 shows the details of the virtual data centre of the open nebula. We have created a virtual data centre using open nebula and implemented our prosed system on open nebula virtual data centre. RNN and ANN are the two extra successive deep learning techniques that were additionally created. Table 1 shows the open nebula virtual data centre setup details.
Table 1 Open nebula virtual data centre details
| No of Instances | Instance Type | vCPU | RAM (GiB) | Storage | OS |
| 2 | Large | 8 | 64 | 1500GB | Centos |
| 4 | Medium | 4 | 32 | 1000GB | Centos |
| 8 | Small | 2 | 32 | 500GB | Centos |
| Authentication | X509 | ||||
| Hypervisor | Kernel-based Virtual Machine | ||||
Table 2 State and age group of the dataset
| State | Age Group | ||
| The total U.S. | Maine | North Dakota | 12 or Older Estimate |
| Northeast | Maryland | Ohio | 12 or Older 95% CI (Lower) |
| Midwest | Massachusetts | Oklahoma | 12 or Older 95% CI (Upper) |
| South | Michigan | Oregon | 12–17 Estimate |
| West | Minnesota | Pennsylvania | 12–17 95% CI (Lower) |
| Alabama | Mississippi | Rhode Island | 12–17 95% CI (Upper) |
| Alaska | Missouri | South Carolina | 18–25 Estimate |
| Arizona | Montana | South Dakota | 18–25 95% CI (Lower) |
| Arkansas | Nebraska | Tennessee | 18–25 95% CI (Upper) |
| California | Nevada | Texas | 26 or Older Estimate |
| Colorado | New Hampshire | Utah | 26 or Older 95% CI (Lower) |
| Connecticut | New Jersey | Vermont | 26 or Older 95% CI (Upper) |
| Delaware | New Mexico | Wyoming | 18 or Older Estimate |
| District of Columbia | New York | Virginia | 18 or Older 95% CI (Lower) |
| Florida | North Carolina | Washington | 18 or Older 95% CI (Upper) |
| Georgia | Iowa | West Virginia | |
| Hawaii | Kansas | Wisconsin | |
| Idaho | Kentucky | Illinois | |
| Indiana | Louisiana | ||
Evaluate the performance of the prosed system, and we have used the National Survey on Drug Use and Health dataset (NSDUH). NSDUH use and functional behaviour at the national, state, and sub-state levels. NSDUH information likewise helps to recognize the degree of substance use and psychological sickness among various sub-gatherings, gauge inclines after some time, and decide the requirement for treatment administrations. Table 2 shows the data collected from the different states and different age groups used in our assessment. Table 3 shows the substance use and mental disorder data set that are used in our experiment.
Table 3 Substance use and mental disorder data
| S.No | Substance Use and Mental Disorders |
| 1 | Illicit drug use in the past month |
| 2 | Perceptions of high risk from smoking |
| 3 | Ache reliever misappropriation in chronological year |
| 4 | Alcohol use in the past month |
| 5 | Tobacco product use in the past month |
| 6 | Cigarette use |
| 7 | Observations of prodigious risk from smoking one |
| 8 | Demanding but not getting treatment at a speciality facility for substance use |
| 9 | Severe emotional disease in the past year |
| 10 | Any Mental Illness in the past year |
| 11 | Received mental health services |
| 12 | Had severe thoughts of suicide |
| 13 | Major depressive episode |
We have conducted six different tests for evaluating the proposed algorithm, performances for test-1, we have used with 5,000 users data, and test-2. We have considered 10,000 users’ medical data. Test-3 we have increased Test-2 users data by adding 2,000 users. Test-4, Test-5 and Test-6 we have assigned 20,000, 25,000 and 30,000 users health data. We have conducted different tests to shows our algorithm works. Even if you increase the data set or decrease the data set, our algorithm gives better performance in terms of delay time. Examination of the outcomes from the three consecutive models appears in Tables 4–7. Figures 5 and 6 depict the uptime delay and downtime delay of different machine learning methods based on the presented infrastructure. We evaluated the delay time of the proposed system. The delay time of the proposed system can be calculated based on the following formula.
Where
UP-Time: Time delay of uploading sensed data to the cloud
Process-Time: Delay of data preprocessing and analytics
Down-Time: Time delay of delivering results to end consumers
All RNNs have loops in the repetitive layer. This gives them a chance to keep up data in ‘memory’ after some time. Be that as it may, it very well may be hard to prepare standard RNNs to take care of issues that require adapting long haul transient conditions. LSTM systems are a sort of RNN that utilizations different units, notwithstanding standard units. LSTM units incorporate a ’memory cell’ that can keep up data in memory for significant periods. Many doors are utilized to control when data enters the memory, when its yield, and when is it slipped, it is mind. This design gives them a chance to adapt to longer-term conditions.
Table 4 UP-time of different machine learning method in (milliseconds)
| Method | TEST1 | TEST-2 | TEST-3 | TEST-4 | TEST-5 | TEST-6 |
| ANN | 400 | 427 | 367 | 396 | 474 | 426 |
| Simple RNN | 312 | 395 | 347 | 297 | 399 | 379 |
| LSTN | 277 | 292 | 287 | 264 | 255 | 312 |
Table 5 Down-time of different machine learning method in (milliseconds)
| Method | TEST1 | TEST-2 | TEST-3 | TEST-4 | TEST-5 | TEST-6 |
| ANN | 300 | 311 | 299 | 288 | 312 | 326 |
| Simple RNN | 299 | 263 | 257 | 202 | 299 | 279 |
| LSTN | 177 | 167 | 199 | 185 | 155 | 200 |
Table 6 Process time of different machine learning method in (milliseconds)
| Method | TEST1 | TEST-2 | TEST-3 | TEST-4 | TEST-5 | TEST-6 |
| ANN | 360 | 371 | 384 | 369 | 342 | 326 |
| Simple RNN | 299 | 300 | 312 | 302 | 299 | 287 |
| LSTN | 277 | 271 | 289 | 265 | 269 | 212 |
Table 7 Total time delay of different machine learning method in (milliseconds)
| Method | TEST1 | TEST-2 | TEST-3 | TEST-4 | TEST-5 | TEST-6 |
| ANN | 1060 | 1109 | 1050 | 1053 | 1128 | 1078 |
| Simple RNN | 910 | 958 | 916 | 801 | 997 | 945 |
| LSTN | 731 | 730 | 775 | 714 | 679 | 724 |
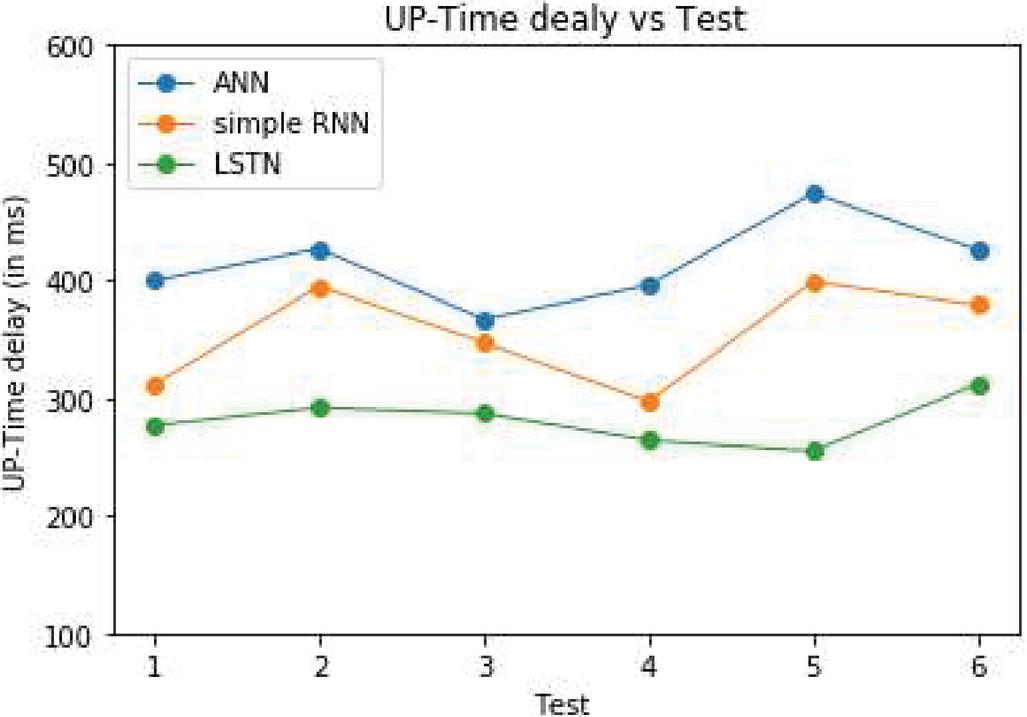
Figure 5 Comparison of UP-time delay with the different deep learning methods.
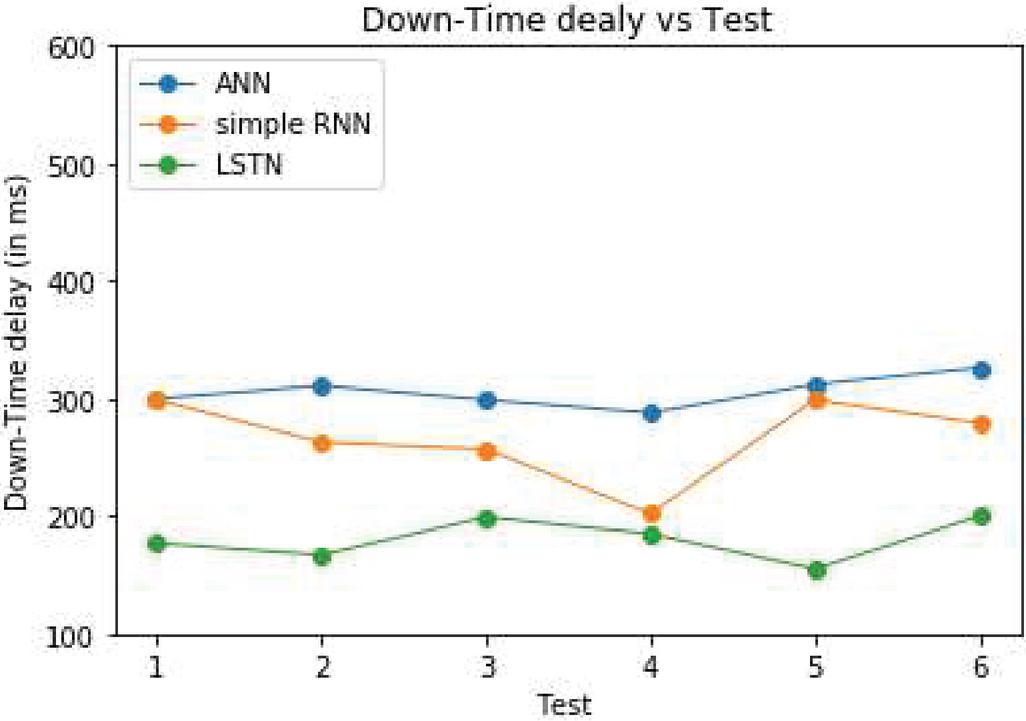
Figure 6 Comparison of downtime delay with the different deep learning methods.
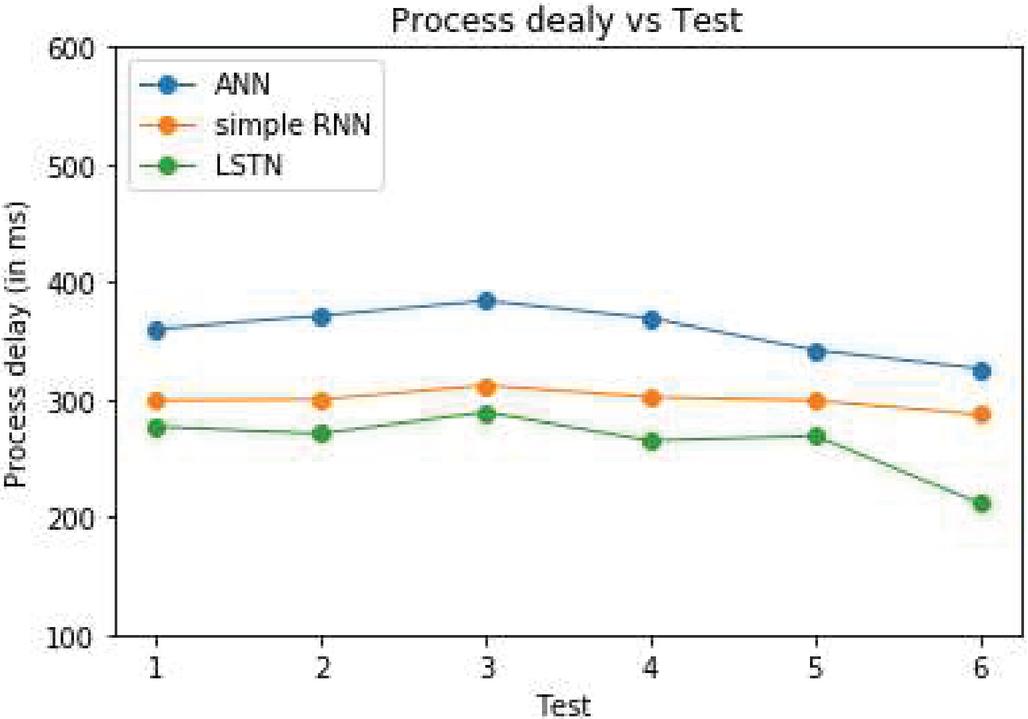
Figure 7 Comparison of process delay with the different deep learning methods.
Figure 7 shows the comparison of process delay with different learning methods such as ANN, RNN, and LSTN. The X-axis represents the number of tests conducted, and the y-axis represents the processing delay. The minimum number of tests conducted was one, and the maximum number of tests conducted was 6. For each test, we have changed the test input data. All RNNs have feedback circles in the intermittent layer. This gives them a chance to keep up data in ‘memory’ after some time. However, it may be hard to prepare standard RNNs to take care of issues that require adapting long haul transient conditions. This is because the slope of the misfortune work rots exponentially with time. Simple RNN performance is between ANN and LSTN. LSTN provides intensive gap length, so it takes minor processing delay than simple RNN and ANN machine learning methods.
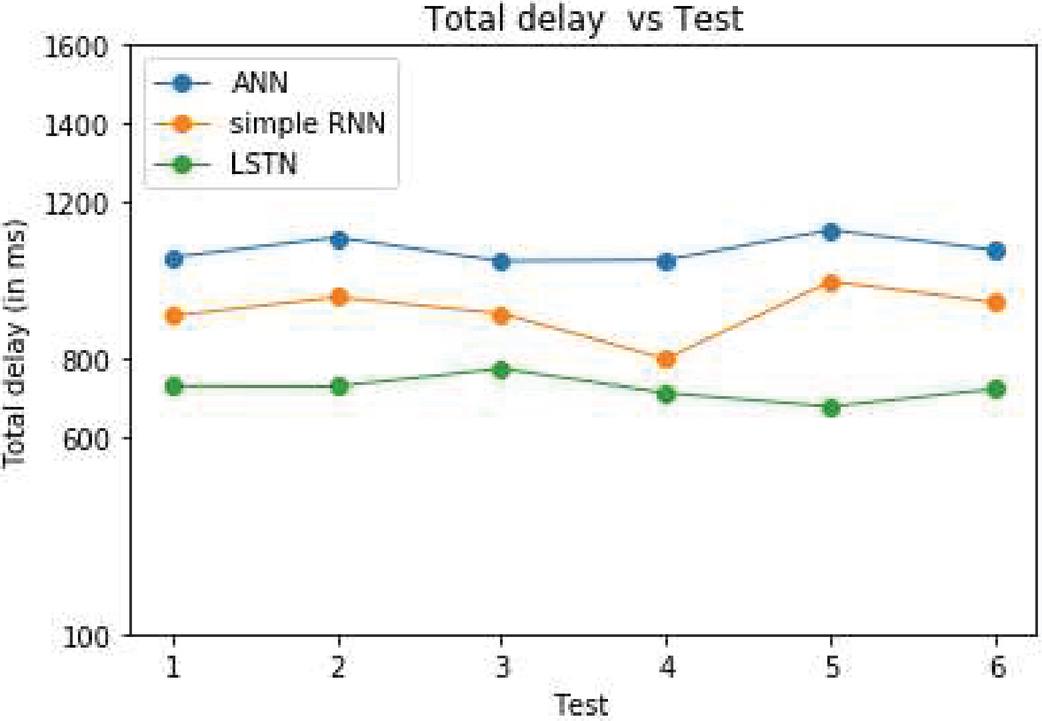
Figure 8 Comparison of a total time delay with the different deep learning methods.
Figure 8 depicts the comparison delay time of different machine learning methods. The X-axis represents the number of tests conducted in different machine learning methods. The y-axis represents time delay in ms seconds. Moreover, take a fixed input and use it to anticipate some fixed measured yield. For instance, one may take a estimated picture and produce a solitary Boolean yield like whether the picture contains a feline. A system like that could not accept some other estimated photo as information. Shockingly basic ANNs like these cannot take inputs that are variable lengths like content, similar to a picture of obscure size or a sentence of indefinite period. There are different systems to construct systems to take variable sizes inputs, one of which is RNNs. RNNs are commonly utilized for grouping information like content, sound, video. So forth, furthermore, they are neural systems that feed their yield over into their sources of info recursively. Even though the RNNs benefit from coding the conditions between inputs, it causes detonating and disappearing against their angle for long information successions. Since both LSTM and RNN can take data from the past context, LSTM takes less time to process the input than simple RNN and ANN machine learning methods.
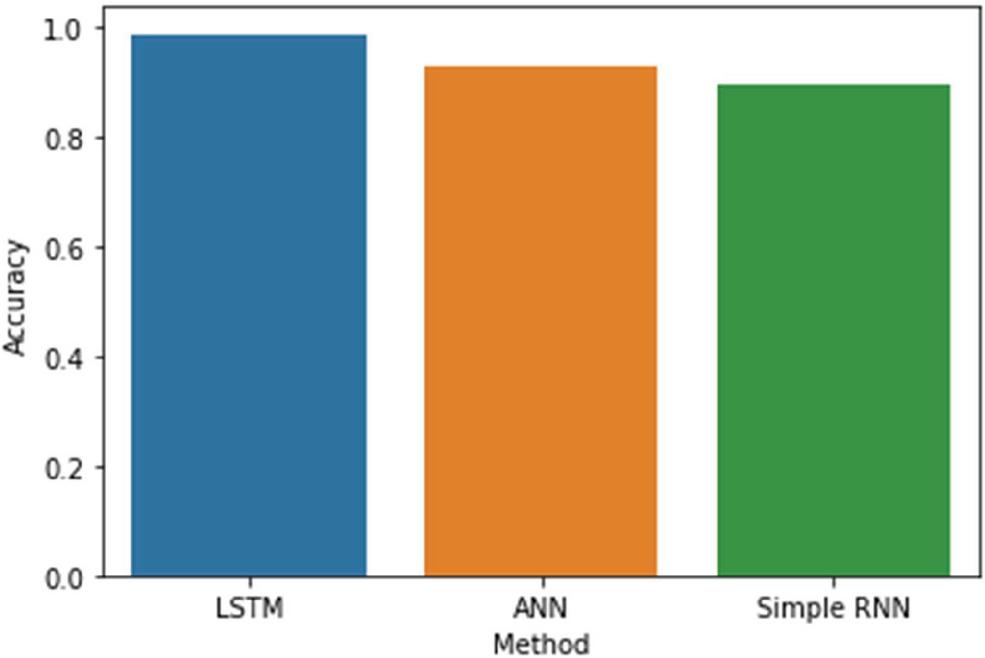
Figure 9 Comparison of accuracy with the different deep learning methods.
The accuracy of the model is calculated with the help of the mental disorder data. Figure 9 depict the accuracy of different deep learning model with the proposed algorithm. LSTM method gives 98 per cent accuracy because of the LSTM characteristics. LSTM is more suitable for the time series data-based prediction. The proposed LSTM takes the user’s time series data and predicts the users’ health status. Simple RNN and ANN give the accuracy of 92 percentage and 89 percentage. It can be decided that the LSTM based is most suitable for the healthcare classification problem and implemented in real-time circumstances.
5 Conclusion and Future Scope
This paper has proposed intelligent personal health monitoring and guidance using long short-term memory for predicting user behaviours, emotion detections, and potential diseases. The main contribution of this paper is that we have designed the IPHMG score model, which will help the proposed system predict the exact emotion and behaviours of the users. Fathomer, we have created an Android application that facilitates interaction between the patients and the system, where the patients seek advice, diagnosis, and treatment. It avoids the side effects that occur to humans on taking medicines without a doctor’s suggestion. It also lists the cases of medical emergencies where doctor intervention is needed. In cases of medical emergencies, too, the doctor’s antibiotic combination is listed in the applications, thus creating awareness to the self on the treatment. User-friendly, as it saves them time, labour, costs, and lives of the people. In the future, we can extend this work to build up a practical choice emotionally supportive network with a specialist’s information to producing customized wellbeing suggestions for needy mobile users.
References
[1] S. Challa, G. Geethakumari, and C. S. N. Prasad, “Patient data viewer: An Android application for healthcare,” Proc. – 2011 Annu. IEEE India Conf. Eng. Sustain. Solut. INDIAN-2011, 2011.
[2] C. Zhang, “Healthcare Mobile App Development with App Inventor in a Health IT Course,” 2014.
[3] A. Das, F. Mueller, C. Siegel, and A. Vishnu, “Desh: Deep learning for system health prediction of lead times to failure in HPC,” HPDC 2018 – Proc. 2018 Int. Symp. High-Performance Parallel Distrib. Comput., pp. 40–51, 2018.
[4] M. Rezaul Karim, M. Cochez, J. B. Jares, M. Uddin, O. Beyan, and S. Decker, “Drug-drug interaction prediction based on knowledge graph embeddings and convolutional-LSTM network,” ACM-BCB 2019 – Proc. 10th ACM Int. Conf. Bioinformatics, Comput. Biol. Heal. Informatics, pp. 113–123, 2019.
[5] Q. Xue and M. C. Chuah, “Explainable deep learning-based medical diagnostic system,” Smart Heal., 2019.
[6] M. Chen, Y. Hao, K. Hwang, L. Wang, and L. Wang, “Disease Prediction by Machine Learning over Big Data from Healthcare Communities,” IEEE Access, vol. 5, no. c, pp. 8869–8879, 2017.
[7] A. Rawal and R. Miikkulainen, “Evolving deep LSTM-based memory networks using an information maximization objective,” GECCO 2016 – Proc. 2016 Genet. Evol. Comput. Conf., pp. 501–508, 2016.
[8] C. Feng et al., “Deep Learning Framework for Alzheimer’s Disease Diagnosis via 3D-CNN and FSBi-LSTM,” IEEE Access, vol. 7, pp. 63605–63618, 2019.
[9] Q. Xue and M. C. Chuah, “New attacks on RNN based healthcare learning system and their detections,” Smart Heal., vol. 9–10, pp. 144–157, 2018.
[10] K. Lohani and D. Mukhopadhyay, “Reduction of medication errors while prescribing using evidence-based treatment,” Int. Conf. Adv. Comput. Commun. Control 2017, ICAC3 2017, vol. 2018–January, no. February 2018, pp. 1–6, 2018.
[11] C. Pasupathi and V. Kalavakonda, “Evidence-Based health care system using Big Data for disease diagnosis,” Proceeding IEEE – 2nd Int. Conf. Adv. Electr. Electron. Information, Commun. Bio-Informatics, IEEE – AEEICB 2016, pp. 743–747, 2016.
[12] S. Series and D. Report, “An Adaptive Evidence-Based Medicine System Based on a Clinical Decision Support System,” vol. 4, no. 11, pp. 160–172, 2012.
[13] M. Abouzahra, K. Sartipi, D. Armstrong, and J. Tian, “Integrating data from EHRs to enhance clinical decision making: The inflammatory bowel disease case,” Proc. – IEEE Symp. Comput. Med. Syst., no. July 2009, pp. 531–532, 2014.
[14] M. Chen, Y. Zhang, M. Qiu, N. Guizani, and Y. Hao, “SPHA: Smart Personal Health Advisor Based on Deep Analytics,” IEEE Commun. Mag., vol. 56, no. 3, pp. 164–169, 2018.
[15] S. Sakr and A. Elgammal, “Towards a Comprehensive Data Analytics Framework for Smart Healthcare Services,” Big Data Res., vol. 4, no. May, pp. 44–58, 2016.
[16] V. Vijayakumar, D. Malathi, V. Subramaniyaswamy, P. Saravanan, and R. Logesh, “Fog computing-based intelligent healthcare system for the detection and prevention of mosquito-borne diseases,” Comput. Human Behav., vol. 100, pp. 275–285, 2019.
[17] M. Bhatia and S. K. Sood, “An intelligent framework for workouts in gymnasium: M-Health perspective,” Comput. Electr. Eng., vol. 65, pp. 292–309, 2018.
[18] P. C. Hii and W. Y. Chung, “A comprehensive ubiquitous healthcare solution on an Android mobile device,” Sensors, vol. 11, no. 7, pp. 6799–6815, 2011.
[19] M. Khovrichev, L. Elkhovskaya, V. Fonin, and M. Balakhontceva, “Intelligent Approach for Heterogeneous Data Integration: Information Processes Analysis Engine in Clinical Remote Monitoring Systems,” Procedia Comput. Sci., vol. 156, pp. 134–141, 2019.
[20] B. Yong et al., “IoT-based intelligent fitness system,” J. Parallel Distrib. Comput., vol. 118, pp. 14–21, 2018.
[21] J.-C. Ni, C.-S. Yang, J.-K. Huang, and L. C. Shiu, “Combining Non-Invasive Wearable Device and Intelligent Terminal in HealthCare IoT,” Procedia Comput. Sci., vol. 154, pp. 161–166, 2019.
[22] A. Akbulut, E. Ertugrul, and V. Topcu, “Fetal health status prediction based on maternal clinical history using machine learning techniques,” Comput. Methods Programs Biomed., vol. 163, pp. 87–100, 2018.
[23] Z. Ni, A. C. Yuksel, X. Ni, M. I. Mandel, and L. Xie, “Confused or not confused?: Disentangling Brain activity from EEG data using Bidirectional LSTM Recurrent Neural Networks,” ACM-BCB 2017 – Proc. 8th ACM Int. Conf. Bioinformatics, Comput. Biol. Heal. Informatics, pp. 241–246, 2017.
[24] A. Smith, K. de Salas, I. Lewis, and B. Schüz, “Developing smartphone apps for behavioural studies: The AlcoRisk app case study,” J. Biomed. Inform., vol. 72, pp. 108–119, 2017.
Biographies

S. Velliangiri obtained his Bachelor’s in Computer Science and Engineering from Anna University, Chennai. Master’s in Computer Science and Engineering from Karpagam University, Coimbatore and Doctor of Philosophy in Information and Communication Engineering from Anna University, Chennai. Currently he is working as Associate Professor in B V Raju Institute of Technology, Narasapur, Telangana. He was a member of Institute of Electrical and Electronics Engineers (IEEE) and International Association of Engineers (IAENG). He is specialized in Network security and Optimization techniques. He has published twenty five International journals and presented ten International conferences. He has authored and co-author of several books. He served as Area Editor in EAI Endorsed journal of Energy Web (Scopus) and Journal of computer science bentham (Scopus). He was the reviewer of IET Communication, Elseiver, Taylor and Francis, Springer, Inderscience and other reputed scopus indexed journals.

V. Anbarasu received his B.E. from SVNIT, Surat, Gujarat in Computer Engineering and M.Tech in IT and PhD in CSE from Sathyabama University, Chennai in 2006 and 2014 respectively. Presently he is working as Associate Professor in the Department of Computer Science & Engineering, SRM University, Chennai. Dr. V. Anbarasu also having 15 years of work experience in Engineering Colleges around India. He has published 11 National & International Journals and 31 Conference publications, attended various workshops, seminars and delivered lectures in workshops during his career. Also acting as a Guest Faculty in BITS, Pilani and taken various offline/online courses like OOPs, Advanced Programming Techniques, Operating System, OOAD, Software Architecture, Computer Graphics, Cryptography etc for WILP with WIPRO. His area of interest includes Human Computer Interaction, IoT, Machine Learning, Algorithms, Cryptography and Security.

P. Karthikeyan obtained his the Bachelor of Engineering (B.E.,) in Computer Science and Engineering from Anna University, Chennai, and Tamil nadu, India in 2005 and received his Master of Engineering (M.E.,) in Computer Science and Engineering from Anna University, Coimbatore India in 2009. He has completed Ph.D. degree in Anna University, Chennai in 2018. Skilled in developing projects and carrying out research in the area of Cloud computing and Data science with the programming skill in Java, Python, R and C. He published more than 20 International journals with good impact factor and presented more than 10 International conferences. He was the reviewer of Elsevier, Springer, Inderscience and reputed Scopus indexed journals. He is acting as editorial board members in EAI Endorsed Transactions on Energy Web, The International Arab Journal of Information Technology and Blue Eyes Intelligence Engineering and Sciences Publication journal.

S. P. Anandaraj received B.E. (CSE) degree from Madras University, Chennai in the year 2004, M.Tech (CSE) with Gold Medal from Dr. MGR Educational and Research Institute, University in the year 2007 (Distinction with Honor) and Ph.D in August 2014. He is presently working as Associate Professor CSE in Presidency University, Bangalore. He has 15 Years of Teaching Experience. His areas of interest include Information security, Data Science, Machine Learning and Networks. He wrote two book chapters in IGI Global Publications USA. He filled the 4 patents for the growth of research. He has published 50 papers in various national and International Journals, national and International Conferences. He serving as an Editorial members for reputed journals. He also attended many National Workshops/FDP/Seminars etc. He is a member of ISTE, CSI, Member of IACSIT and Member of IAENG.
Journal of Mobile Multimedia, Vol. 18_2, 349–372.
doi: 10.13052/jmm1550-4646.18210
© 2021 River Publishers