Context-aware Based Personalized Recommendation on Mobile for Monitoring Excessive Sugar Consumption of Thai Adolescents
Rodjana Suwan1, Punnarumol Temdee1,* and Ramjee Prasad2
1Computer and Communication Engineering for Capacity Building Research Center, School of Information Technology, Mae Fah Luang University, Chiang Rai, Thailand
2CTIF Global Capsule (CGC), Department of Business Development and Technology, Aarhus University, Denmark
E-mail: rodjana.suw@mfu.ac.th; punnarumol@mfu.ac.th; ramjee@btech.au.dk
*Corresponding Author
Received 23 June 2021; Accepted 04 February 2022; Publication 07 July 2022
Abstract
Given the harmful effects of excessive sugar consumption, everyone should be aware of the amount of sugar they consume in daily life. Generally, managing nutrition and preventing negative effects from sugar intake requires a nutritional specialist or specialized knowledge, which may not always be readily accessible or understandable. Therefore, there is a need for a mobile application that can track excessive sugar consumption. This study proposes a context-aware personalized recommendation mobile application for monitoring excessive sugar consumption and providing individual recommendations (based on a predefined set of 144 rules) to Thai adolescents. The application is user friendly and can be used to provide recommendations to users for sugar consumption and proper exercise each day. Personal, health, and lifestyle data are collected and analyzed to provide individualized recommendations to each user. Experiments were conducted with 140 Thai adolescents aged 15 to 25 years old. Users’ preferences regarding degree of awareness in presentation style were also investigated. Users rated their satisfaction with the proposed mobile application as very high in terms of both function and personalization. In addition, fully automated recommendations were found to be the preferred degree of awareness among the test group.
Keywords: Nutrition, sugar consumption, lifestyle, context-awareness, personalized recommendations.
1 Introduction
Thailand is currently experiencing a health crisis resulting from high rates of sugar consumption among the Thai population, an issue that should be receiving more attention [1]. A majority of the Thai population is at risk of health problems caused by excessive sugar intake, such as diabetes, obesity, hypertension, and vascular diseases [2]. Recent statistics show that Thailand is experiencing an increase in primary chronic diseases that can be prevented by dietary and lifestyle adjustments, such as type 2 diabetes mellitus, type 3 diabetes, cardiovascular and heart diseases, and cancer [3]. The main risk factor related to improper dietary habits is neglecting to consider nutrition profile and consumption amount at each meal. Observations from the Ministry of Public Health [4] indicate that most Thai teenagers consume more than 20 tablespoons of sugar each day—three times more than the recommended amount. The Ministry found that most Thai people consume sugar in the form of sweetened beverages and condiments in excess of the standards [5] established by the Ministry of Public Health [4]. As a result, Thai teenagers tend to have a high body mass index (BMI). In 2017, teenagers from 27,960 households in Thailand consumed excessive amounts of sugar in their daily meals [5]. Therefore, Thai teenagers need to be aware of their daily sugar consumption and strictly control their dietary habits to prevent the onset of related chronic diseases.
Lack of knowledge about nutritional information makes healthy consumption choices more challenging. However, technology can be used to facilitate the work of doctors and patients. For instance, mobile applications have been developed with which patients can record personal information, consumption data, personal activity, and bloodwork results, allowing experts to verify patients’ personal information and behavioral data and make patients feel as though a doctor is always there to advise and monitor them. The system was created to help predict the occurrence of various abnormalities that may surface, allowing doctors to promptly treat those abnormalities [6]. Other applications have been developed to monitor, control, and make consumption recommendations for diabetic patients [7–9]. However, patient adherence must be strict for these applications to be effective, and they are often not tailored for adolescent users. Moreover, some are designed for the general public [10, 11] or do not make specific recommendations regarding sugar and carbohydrate intake.
Consequently, this study proposes a mobile application designed to monitor excessive sugar consumption and provide personalized recommendations to guide users in controlling their excess sugar and carbohydrate intake before they suffer negative health effects. This study employs a multi-nutritional criteria decision model [12] consisting of a predefined set of 144 rules based on the analysis of personal, health, and lifestyle data under a nutritionist’s supervision. Recommendations, including suggestions regarding sugar consumption and exercise, are provided to the user based on the context-awareness principle. The efficiency and user satisfaction of the proposed mobile application was evaluated in testing with 140 Thai adolescents aged between 15 and 25 years old. Users’ preferences regarding degree of awareness in terms of the presentation style of the mobile application were also investigated.
2 Literature Review
This section summarizes some existing work related to this study in the areas of mobile applications, context-aware recommendations, and personalized recommendations in healthcare.
2.1 Mobile Applications in Healthcare
As people are now carrying their mobile phones for almost the entire day, portable devices have become an extraordinary source of information, including in the healthcare domain [13]. The utilization of smartphones and tablets has empowered consumers and entrepreneurs and transformed how people access information and consume services. Nowadays, these technologies are poised to alter the healthcare field in terms of service delivery and patient experience [14]. Many healthcare providers use mobile applications to provide quality healthcare services and collect user data for further utilization. Recently, mobile applications designed to facilitate the treatment and diagnosis processes have been widely developed and employed. For example, a mobile application framework called SleepCare has been proposed for screening and managing the sleep cycle [15]. Many mobile applications have been developed for self-management purposes, especially for chronic conditions such as diabetes [9, 16, 17] and cardiovascular disease [18]. For diabetes, mHealth [9] is an important example. This mobile application focuses on self-management of medical care for diabetes patients and provides necessary related functions, such as heart rate monitoring and vaccination scheduling. In the area of cardiovascular disease, the Cardiac app [18] was developed to detect and record a person’s heart rate. Cardiac can be used with a smart wearable device to monitor body temperature and heart rate and send data to a server to prevent emergencies [18]. Mobile applications are also widely used for mental health services. For example, the WHAAM application [19] aims to monitor the behaviors of patients with attention deficit hyperactivity disorder. The application provides tools for evaluating the efficacy of interventions as well as data collection. Gamification in mobile applications also typically increases users’ engagement during the treatment process [20].
Mobile applications are also widely employed for general health promotion. Many applications have been developed with the aim of promoting users’ well-being [21], especially with regard to diet. Within this category of mobile applications, tools that can monitor eating behavior and provide users with nutrition information are very popular. For example, eDietary Portal [22], iFood [11], and WellCo [23] can be used to manage daily calorie consumption and provide suggestions regarding diet and exercise. The mobile application proposed in this study also aims to promote users’ well-being. Rather than monitoring calorie consumption, however, the proposed mobile application monitors sugar and carbohydrate consumption. It is specifically designed and developed for Thai adolescents, who tend to consume excessive amounts of sugar in their daily lives.
2.2 Context-Aware Recommendations in Healthcare
Context-aware computing has been widely introduced in many application areas, especially in the healthcare domain. These applications are very sensitive to the context (i.e., any information that can be used to characterize the users and the situation) [24]. Context awareness relates directly to a system’s adaptability [25], which can be demonstrated in various ways, such as its functionality, delivered data and services, or user interface. Context-aware systems and applications change their behaviors based on the context of the user and the situation. Recently, recommendation systems, a type of context-aware application, have received extensive attention. Context-aware recommendation systems combine contexts and user statuses to execute systems or applications [26, 27].
Generally, a recommendation system is used to tailor products and services to individual users. In the realm of healthcare applications, recommendation systems are widely used in various health-related processes. For example, a system called DIETOS provides individualized nutritional advice to enhance the quality of life of patients with diet-related chronic diseases during the treatment process [28]; E-CARE was introduced to promote remote e-healthcare services, classified into three divisions (primary, secondary, and emergency) [29]; and a system called ADAPT provides context-aware solutions for personalized asthma management [30].
With regard to prevention, the provision of context-aware recommendations for monitoring patients with multiple health conditions is highly prevalent. For example, a self-configuring mobile application using a context-aware architecture [31] was developed for monitoring health and cardiac arrhythmias, including tachycardia and bradycardia, in different situations [32]. The recommended systems in actual situations use clinical data as important contextual information to predict heart failure [33] and monitor hypertensive heart disease [32]. Among the variety of application types, mobile applications can introduce live monitoring tools, which have many advantages, such as coping with dynamic changes and promoting mobility [34]. Many context-aware recommendation systems target older populations and patients and provide monitoring and other services based on the guidance of health experts [36–38]. However, context-aware recommendation systems for healthcare applications have not yet widely been developed for young people, which is the main objective of this study.
2.3 Personalized Recommendations in Healthcare
Context-aware recommendation systems that are designed to provide any response to an individual user can be called personalized recommendation systems [38]. Nowadays, many products and services are delivered to customers in a manner that utilizes recommendation systems to provide greater individualization. These systems rely on the analysis of personal historical data, among other datasets, to identify suitable products, courses, or services [23]. Recommendation systems can reduce the time required to explore the needed data [23, 39]. In healthcare services, many healthcare providers have applied personalized recommendation systems to understand patients’ health conditions and suggest personalized healthcare services to each person [41–44]. Personalized recommendation systems can empower patients’ self-monitoring by notifying them of and suggesting appropriate individual healthcare programs, such as medical services and treatment plans [41–43]. In addition, recommendation systems use factors related to users that are collected from applications or smart devices.
In the healthcare domain, three different types of data are normally used in recommendation systems: personal, health, and lifestyle. Personal data are those that represent an individual in general. Health data include measurements related to health conditions, such as BMI, heart rate, and blood pressure. Lifestyle data typically include habits, hobbies, and consumption and exercise behaviors [41–44]. For exercise applications, personalized recommendation systems provide individual programs to help users properly manage their daily life activities [44]. These applications normally require personal, health, and lifestyle data to provide these individualized programs [10, 45–49]. Recently, some mobile applications have employed the context-awareness principle to provide personalized programs to individual users [45]. However, it is still challenging for any mobile application to succeed in engaging users.
Although dietary-related mobile applications have also recently been widely used, few exist that are specifically designed for monitoring excessive sugar consumption among adolescents. The World Health Organization (WHO) and the Food and Agricultural Organization have stated that sugar and other carbohydrate-containing foods play an indispensable role in balancing dietary health [49]. Although there is no evidence that sugar consumption directly causes lifestyle-related health problems such as obesity, heart disease, diabetes, and cancer [49], an improper lifestyle, along with personal health status, can result in a greater impact on the consumption of sugar on personal health.
Therefore, this study proposes a mobile application that is specifically designed for monitoring Thai adolescents’ excessive sugar consumption and providing individualized suggestions. Following the principle of context awareness, personal, health, and lifestyle data are used as the main contexts for providing the personalized recommendations in this study. The multi-criteria decision model [12], presented as a predefined set of rules, is used together with the context-awareness principle to provide personalized recommendations. The proposed mobile application was evaluated in terms of user satisfaction with functions and personalization support. The study also evaluated users’ preferred degree of awareness in presentation style to determine the appropriate presentation for engaging Thai adolescents.
3 Methodology
Three processes were involved in the methodology of this study: algorithm design, mobile application development, and mobile application evaluation (Figure 1).

Figure 1 Research methodology.
More detail regarding each process is presented below.
3.1 Algorithm Design
The proposed recommendation model consists of two elements: content and presentation style (Figure 2). The content is analyzed based on the multi-nutritional criteria decision model [12] and expert advice. The presentation style is proposed based on the context-awareness principle. Details are provided in this section.
Figure 2 Conceptual diagram of context-aware recommendation system.
3.1.1 Multi-nutritional criteria decision model
The multi-nutritional criteria decision model [12], shown in Figure 2, is used to determine whether individuals require recommendations regarding their sugar consumption. This model collects nutrition facts and nutritionists’ recommendations to create a recommendation that best matches the individual. The model considers each criterion when making a decision. The data used to construct the model include personal, health, and lifestyle data (see Table 1). Personal data include gender and age; health data include BMI and any diseases; and lifestyle data were collected through questionnaires (Q1–Q20). The model, presented as a predefined set of 144 rules using a decision tree, was constructed based on data collected from 349 Thai adolescents aged between 15 and 25 years [12]. The collected data are randomly selected from an online questionnaire. The included study received an ethical approval certificate from the university. The details of the collected data and their values are presented in Table 1.
Table 1 Collected data and values
| Collected Data | Values |
| Gender | Male; female |
| Age (years) | 15–18; 19–22; 23–25; 25 |
| BMI | Weight (kg); height (cm) |
| Personal diseases | High obesity; heart disease; depression; type 2 diabetes; no disease; other |
| Limiting daily sugar (Q1) | Scored on five-point Likert scales |
| Looking for nutrient content on product labels (Q2) | |
| Limiting high-cholesterol food (Q3) | |
| Eating at least five different types of fruits per day (Q4) | |
| Avoiding alcoholic drinks (Q5) | |
| Avoiding smoking (Q6) | |
| Avoiding fast food (Q7) | |
| Avoiding soft drinks (Q8) | |
| Avoiding desserts (Q9) | |
| Engaging in hobbies in free time (Q10) | |
| Engaging in frequent exercise (Q11) | |
| Being healthy (Q12) | |
| Getting enough sleep (Q13) | |
| Preferring to eat fermented foods (Q14) | |
| Adding sugar every time (Q15) | |
| Loving food consumption (Q16) | |
| Having meals on time (Q17) | |
| Adding sugar to tea or coffee (Q18) | |
| Preferring online food delivery (Q19) | |
| Being inspired in food selection (Q20) |
Lifestyle data (Q1–Q20; see Table 1) can be classified into six groups according to the categories of the various criteria [50]: healthy choices (Q1–Q4, Q14, Q18); harm avoidance (Q5–Q9); daily routine (Q15–Q17); physical exercise (Q10–Q12); psychological health (Q13); and common behaviors (Q19–Q20). In this study, five-point Likert scales were used to assess both satisfaction and frequency. This study adopted the classification rules from previous work [12]. Example rules used in this study are shown in Table 2. The output decision comprises two classes: “Yes” and “No.” The “Yes” class means that the user needs recommendations regarding sugar consumption, whereas the “No” class means that the user does not need such recommendations.
Table 2 Example classification rules
| Rule No. | Definition |
| 1 | If Q14 value 2.5 points and BMI value 23.8 kg/m and Q3 value 3.5 points, then Recommendation = Yes |
| 2 | If Q14 value 2.5 points and BMI value 23.8 kg/m and Q3 value 3.5 points and Q17 value 2.5 points, then Recommendation = No |
| 3 | If Q14 value 2.5 points and BMI value 23.8 kg/m and Q3 value 3.5 points and Q17 value 2.5 points and Q7 value 4.5 points, then Recommendation = Yes |
| 4 | If Q14 value 2.5 points and BMI value 23.8 kg/m and Q3 value 3.5 points and Q17 value 2.5 points and Q7 value 4.5 points, then Recommendation = No |
| 5 | If Q14 value 2.5 points and BMI value 23.8 kg/m and Q18 value 4.5 points and Q4 value 3.5 points, then Recommendation = Yes |
| 44 | If Q14 value 2.5 points and Q6 value 1.5 points and Q15 value 1.5 points and Q18 value 4 points and Q16 value 2.5 points and BMI value 23.4 kg/m and Q3 value 4.5 points and Q18 2.5 points and BMI 17.2 kg/m, then Recommendation = No |
For example, Rule 1 (see Table 2) declares that users require recommendations from the system to control their sugar consumption if they have an agreement value of more than 2.5 points for the statement that they prefer to eat fermented food (Q14), a BMI over 23.8 kg/m, and an agreement value of more than 3.5 points for the statement that they limit high-cholesterol foods (Q3). Rule 2 declares that users do not require recommendations from the system to control their sugar consumption if they have an agreement value of more than 2.5 points for the statement that they prefer to eat fermented food (Q14), a BMI over 23.8 kg/m, an agreement value less than or equal to 3.5 points for the statement that they limit high-cholesterol foods (Q3), and an agreement value of more than 2.5 points for the statement that they have their meals on time (Q17).
Individuals who require recommendations will be provided with individualized content in different presentation styles. The details of these two processes are shown as follows.
3.1.2 Context awareness for mobile applications
Context awareness refers to a system’s ability to consider an entity’s situation by using context [51, 52]. Contextual information may include data obtained from the user or a smart device regarding the specific circumstances. In this study, context awareness is used to design an appropriate degree of awareness and provide different types of recommendation presentation styles to users that best match their preferences. The degree of awareness is evaluated in this study to determine the most suitable presentation style for the target group of Thai adolescents. Three types of recommendation systems are investigated in this study, described below.
Fully Automatic Recommendations
A fully automatic recommendation system is self-adaptive, adjusting its behavior in accordance with its perception of the environment. Such systems require little or no effort from users, and no special knowledge is necessary to use them [53, 54]. In this study, fully automatic recommendations are automatically provided recommendations for sugar and carbohydrate consumption based on the system’s calculation of the user’s consumption given the information that the user enters into the application (see Table 1), without any intervention from the user.
Partially Automatic Recommendations
Partially automatic recommendation systems require involvement from the user to specify how the application should change or behave in some situations. The system can provide all possible information or actions to the user so that the user can select which actions are appropriate [55]. Such systems are designed such that users can choose a word from the system. For partially automatic recommendations, the system provides automatic carbohydrate intake recommendations based on its calculations. However, it also allows users themselves to calculate and enter the amount of added sugar that they want to consume per day, thereby enabling the system to be flexible in adjusting to the needs of users and allowing them to participate in some decisions.
Zero Automatic Recommendations
For systems that provide zero automatic recommendations, recommendations are provided only based on what the user has set and entered into the system. Such systems allow users to decide all of their consumption goals and recommendations based only on user input. Thus, users are empowered to determine their own consumption and to decide what is best suited to their needs. However, users’ predefined goals will be based on specific guidelines set by nutritionists.
3.1.3 Recommendation design
After the individual is classified as the person requiring the recommendation, the recommendation is constructed based on various factors to suit that user’s specific personal health conditions and lifestyle. The associated variables for each factor are presented in Table 3.
Table 3 Descriptions of all factors: body mass index, physical activity, consumption and lifestyle, and diabetes risk
| No. | Factor | Variable | Description |
| 1 | Body Mass Index (BMI) | BMI1 | Being underweight (less than 18.50 kg/m) |
| 2 | BMI2 | Being a healthy weight (greater than or equal to 18.50 kg/m and less than 23.00 kg/m) | |
| 3 | BMI3 | Being overweight (greater than or equal to 23.00 kg/m) | |
| 4 | BMI4 | Being obese (greater than or equal to 25.00 kg/m) | |
| 5 | Physical Activity(ACT) | ACT1 | Engaging in normal activities and some exercise |
| 6 | ACT2 | Exercising three to five times per week | |
| 7 | ACT3 | Exercising every day | |
| 8 | ACT4 | Engaging in hard exercise every day | |
| 9 | Consumption and Lifestyle(LIF) | LIF1 | Consuming fewer carbohydrates than required (less than 24 g) |
| 10 | LIF2 | Consuming prescribed amount of carbohydrates (less than or equal to 24 g) | |
| 11 | LIF3 | Consuming excessive amounts of carbohydrates (greater than 24 g) | |
| 12 | Diabetes Risk (DIA) | DIA1 | No diabetes |
| 13 | DIA2 | At risk of becoming diabetic | |
| 14 | DIA3 | Diabetic |
The specific details of the recommendations provided in this study are shown in Table 4.
Table 4 Descriptions of recommendations for body mass index, physical activity, consumption and lifestyle, and diabetes risk
| No. | Recommendation | Variable | Description |
| 1 | Recommendations for Body Mass Index(RBMI) | RBMI1 | – Eating good-quality food from adequate range of food groups, focusing on meat, milk, eggs, vegetables, and fruits, getting enough rest |
| 2 | RBMI2 | – Maintaining health and controlling weight at a healthy level, maintaining the same weight |
|
| 3 | RBMI3 | – Limiting foods such as flour, sugar, and fat – Exercising for at least 30 minutes at least three times per week |
|
| 4 | RBMI4 | – Avoiding starchy foods such as sugar and fats – Being active while performing daily tasks such as housework, work, and occupation – Exercising for at least 30 minutes every day |
|
| 5 | Recommendations for Physical Activity(RACT) | RACT1 | – Exercising at least 30 minutes three times per week |
| 6 | RACT2 | – Maintaining exercise regimen – Getting enough rest |
|
| 7 | RACT3 | – Maintaining exercise regimen – Eating good-quality food from adequate range of food groups, focusing on meat, milk, eggs, vegetables, and fruits – Getting enough rest |
|
| 8 | RACT4 | – Maintaining exercise regimen – Eating good-quality food from adequate range of food groups, focusing on meat, milk, eggs, vegetables, and fruits – Getting enough rest |
|
| 9 | Recommendations for Consumption and Lifestyle(RLIF) | RLIF1 | – Maintaining level of food consumption |
| 10 | RLIF2 | – Maintaining level of food consumption |
|
| 11 | RLIF3 | – Reducing sugar consumption – Checking blood sugar levels every year |
|
| 12 | Recommendations for Diabetes Risk (RDIA) | RDIA1 | – Maintaining level of food consumption |
| 13 | RDIA2 | – Moderating level of daily food consumption |
|
| 14 | RDIA3 | – Limiting foods such as flour, sugar, and fat |
All recommendation rules shown in Tables 3 and 4 were approved by two nutrition specialists. The condition of referral in this study refers to the related guidelines in food supplements, and each condition is presented as a factor linked with features related to personal health and lifestyle status.
As shown in the Tables 1 and 3, BMI indicates different balances of body weight and height, based on age and gender, that can be used to control daily energy consumption [56, 57]. BMI, measured in kg/m, is divided into the following categories: underweight (BMI 18.50), healthy weight (18.50 BMI 23.00), overweight (23.00 BMI 25.00), and obese (BMI 25.00). Since blood glucose is one of the primary energy sources for muscle construction during activity, limiting sugar consumption can balance and improve physical performance [58]. Furthermore, the WHO suggests that daily sugar consumption be limited to 24 grams due to the adverse effects of increased prevalence of dental cavities, micronutrient deficiencies, obesity, and diabetes [49]. Excessive sugar consumption increases the risk of high levels of triglycerides, which can heighten cholesterol levels [59]. Thus, these two factors are linked. Soft drink consumption is also associated with undesirable side effects [60]. However, consuming added sugar may be inevitable due to an individual’s personal lifestyle. Personal lifestyle is relevant with regard to sugar consumption among adults insofar as it affects food consumption frequency and schedule [61]. To realize cooperative sugar consumption behavior, the U.S. Food and Drug Administration states that food labeling enables better consideration of health and nutrition contents, even if it does not fit an individual’s personal preferences [62]. As all of these are relevant to user behavior, this study applies the mentioned factors with different classes to cover personal information and create 144 recommendation rules based on a predefined ruleset to match as many users as possible (examples presented in Table 5).
Table 5 Sample recommendation rules
| Rule | Factor Set | Recommendation Set |
| 1 | BMI1 & ACT1 & LIF1 & DIA1 | RBMI1 & RACT1 & RLIF1 & RDIA1 |
| 2 | BMI1 & ACT1 & LIF1 & DIA2 | RBMI1 & RACT1 & RLIF1 & RDIA2 |
| 3 | BMI1 & ACT4 & LIF3 & DIA3 | RBMI1 & RACT4 & RLIF3 & RDIA3 |
| 4 | BMI2 & ACT1 & LIF1 & DIA1 | RBMI2 & RACT1 & RLIF1 & RDIA1 |
| 5 | BMI2 & ACT1 & LIF1 & DIA2 | RBMI2 & RACT1 & RLIF1 & RDIA2 |
| 6 | BMI3 & ACT4 & LIF2 & DIA1 | RBMI3 & RACT4 & RLIF2 & RDIA1 |
| 7 | BMI3& ACT4 & LIF3 & DIA1 | RBMI3 & RACT4 & RLIF3 & RDIA1 |
| 8 | BMI3& ACT4 & LIF2 & DIA2 | RBMI3 & RACT4 & RLIF2 & RDIA2 |
| 9 | BMI4& ACT3 & LIF2 & DIA3 | RBMI4 & RACT3 & RLIF2 & RDIA3 |
| 10 | BMI4& ACT2 & LIF2 & DIA3 | RBMI4 & RACT2 & RLIF2 & RDIA3 |
| 144 | BMI4& ACT4 & LIF3 & DIA3 | RBMI4 & RACT4 & RLIF3 & RDIA3 |
Rule 1 (see Table 5) is assigned to a user who is underweight (BMI 18.50 kg/m), engaging in normal activity and some exercise, consuming fewer carbohydrates than required, and not diabetic. The given recommendation for such a user is to consume quality foods from a range of food groups, with a focus on meat, milk, eggs, vegetables, and fruits, and to get enough rest. The user should also exercise for 30 minutes at least three times per week and maintain adequate levels of food consumption. Rule 144 is given to a person who is obese (BMI 25.00 kg/m), engaging in hard exercise every day, consuming excessive amounts of carbohydrates, and diabetic. The given recommendation for this user is to avoid starchy foods such as sugar and fats; perform active daily tasks such as housework, work, and occupation; and exercise for at least 30 minutes every day. The user should also eat quality foods from each of the required food groups, focusing on meat, milk, eggs, vegetables, and fruits, and get enough rest. This person should also reduce their sugar consumption, check their blood sugar levels every year, and limit foods such as flour, sugar, and fat.
3.2 Mobile Application Development
The system is a mobile application that the users can access via the internet. The application uses a PHP server (version 7.3 or higher) connected to a MySQL database. The application allows users to save their personal data through the Android platform. It subsequently sends these data to be stored and processed on the server and can then access the information to provide recommendations to users in Android applications. The system’s data structure consists of three main parts: personal data, health status, and lifestyle data. These are further divided into personal information, personal disease information, activity information, sugar and carbohydrate consumption information, recommendation information, and daily consumption statistics, all of which were used to create various functions in the algorithm design by linking various processes and data (see Appendix).
3.3 Mobile Application Evaluation
The developed mobile application was evaluated by a group of Thai adolescents aged between 15 and 25 years, including both males and females whose BMIs ranged from 14.88 to 31.99 kg/m and who were accustomed to using technology in daily life. The characteristics of the test group are shown in Table 6.
Table 6 Descriptive characteristics of user testing group
| Measurement | |||
| Factor | Range | Mean | Standard Deviation |
| Age | 15–25 years | 20.81 | 2.2 |
| Gender | Male, female | — | — |
| Weight | 40–90 kg | 57.64 | 12.97 |
| Height | 150–181 cm | 164.25 | 7.72 |
| Body Mass Index | 14.88–31.99 kg/m | 21.25 | 3.93 |
The evaluation addressed two aspects: user satisfaction and preferred degree of awareness. Within the category of user satisfaction, two aspects were evaluated: satisfaction with functions and satisfaction with personalization support. Five-point Likert scales were used for these measures. Satisfaction with each criterion was assessed using five levels, where 1 indicated the lowest satisfaction and 5 the highest. The possible satisfaction levels were categorized as “very high” (4.21–5.00), “high” (3.41–4.20), “medium” (2.61–3.40), “low” (1.81–2.60), and “very low” (1–1.8).
With regard to preferred degree of awareness, users were asked for their preferences regarding content presentation style at three different phases (over the course of seven days). In each phase, the user was required to indicate their preferred content presentation style from three possible levels of degree of awareness: fully automatic recommendations, partially automatic recommendations, and zero automatic recommendations.
4 Experimental Results and Discussion
4.1 User Interface
The proposed mobile application was designed for the Android platform. Example results are presented for each page of the application interface, as follows.
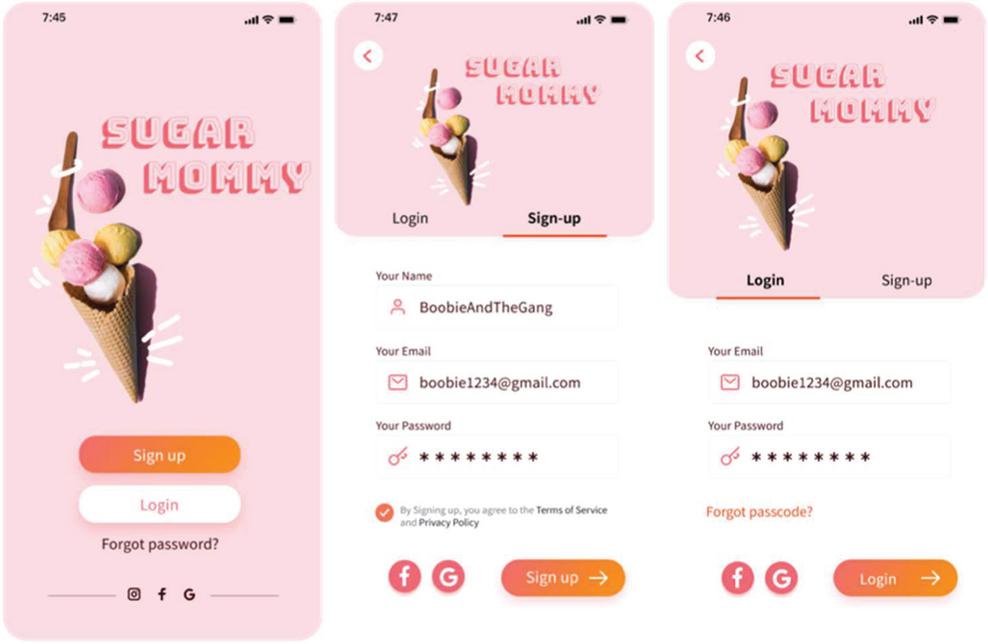
Figure 3 Homepage and login page.
The homepage and login page, shown in Figure 3, allow users to choose to either register a new account or log into the system with a preexisting account. The registration page is used to prove the identity of the user as an authentication requirement.
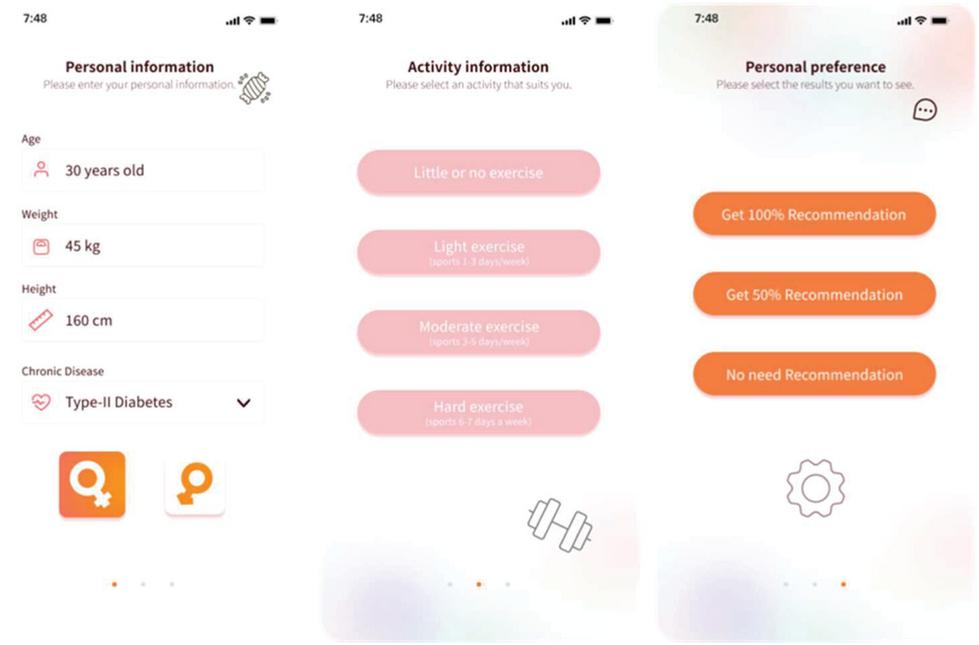
Figure 4 Personal information page.
The personal information page, shown in Figure 4, includes all factors relevant to the multi-nutritional criteria. Users do not need to calculate BMI themselves; the system automatically calculates it based on weight and height. Users are also required to provide authorization for users or administrators to observe the stored information. The activity page allows users to choose the activities that suit them so that the system can evaluate whether the user should be provided recommendations to engage in the selected activity. The personal preference page allows users to design the automation level of the recommendation system based on what kind of recommendations suits their lifestyle. If users select Item 1 (fully automatic recommendations), the system will automatically calculate their carbohydrate intake and direct them to the main page, shown in Figure 5. If users select Item 2 (partially automatic recommendations), the system will allow them to enter their daily consumption of sugar (how many grams they would like to set as their daily consumption limit), as shown in Figure 6(a). The system will then make recommendations according to users’ requirements. If users choose Item 3 (zero automatic recommendations), the system will ask them to enter their daily limit for sugar consumption by themselves and will calculate the amount of carbohydrate intake as required by the user, as shown in Figure 6(b). The system will then make recommendations according to the user’s specifications.
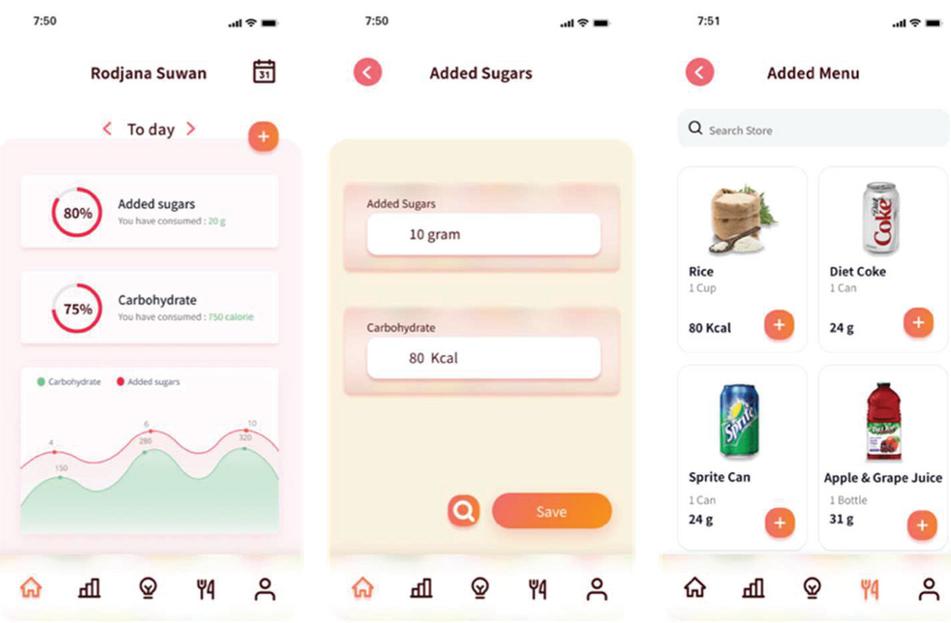
Figure 5 Personal consumption goals page.
The summary page for daily sugar consumption is displayed in Figure 5. Two separate circles are used to indicate added sugars and carbohydrate consumption. Users can press the icon to increase their sugar consumption and can click on the added sugars circle to view or edit their sugar consumption information. When the user presses the icon to increase their sugar consumption level, a page will appear that enables them to fill in the amount of sugar they have consumed, after which they can press the save button to return to the main page. If the user presses the search icon, they are taken to the next page, where they can press the icon if they have consumed any of the items displayed. After users press the icon, they are returned to the main page, and their consumption amount is calculated.
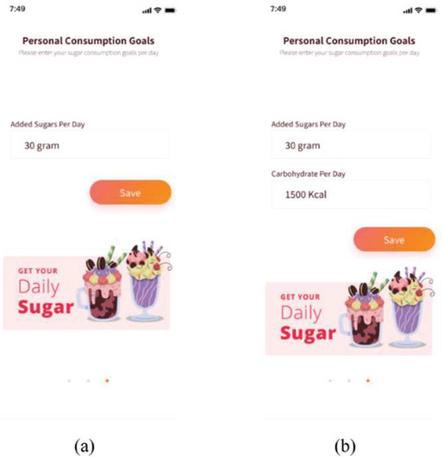
Figure 6 Personal consumption goals page: (a) partially automatic recommendations and (b) zero automatic recommendations.
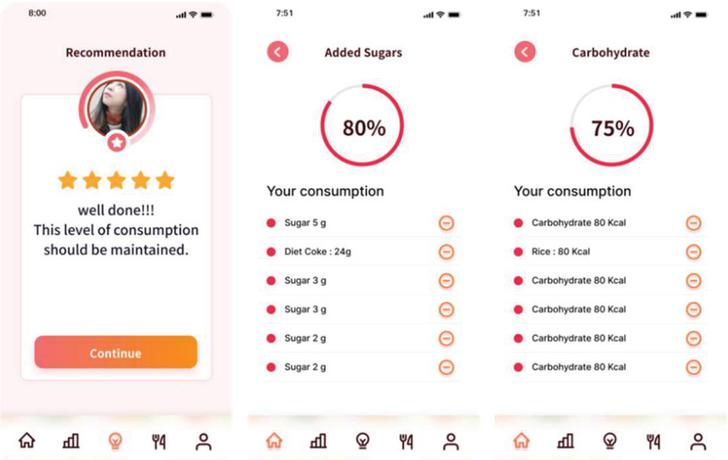
Figure 7 Recommendation level page.
As shown in Figure 7, when it is time for dinner, the system shows a summary of users’ consumption so that they can see whether they have achieved their target for the day. When users press the sugar consumption circle, the sugar consumption details page appears. Users can delete sugar consumption information by pressing the – button if they have entered their consumption incorrectly. When users press the carbohydrate intake circle, the carbohydrate intake details page appears. Users can delete their carbohydrate consumption information by pressing the – button to delete an entry if they have entered their information incorrectly.
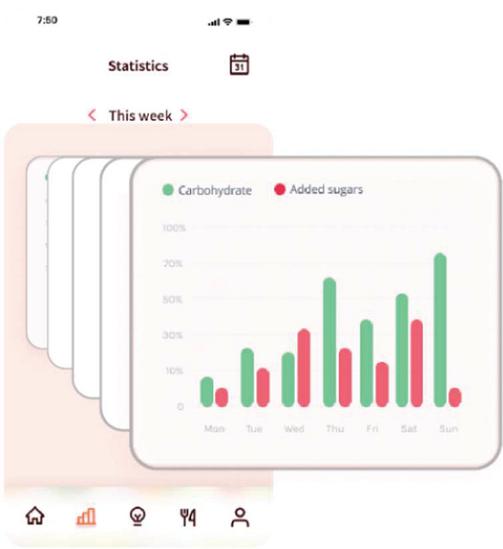
Figure 8 Statistics page.
Users’ weekly statistics for sugar and carbohydrate consumption can be visualized as a graph presented on the statistics page, as shown in Figure 8.
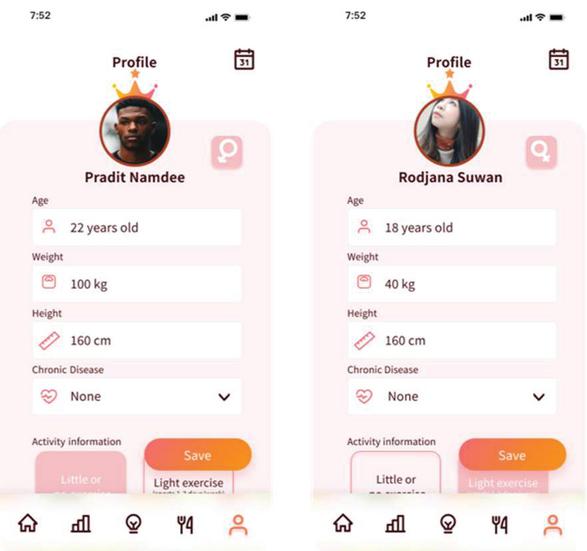
Figure 9 Profile page.
User profile pages, shown in Figure 9, allow users to edit their profiles. If a user has made an incorrect entry or their weight has changed, the system will make calculations based on the various user data recorded in a log to identify the consumption behavior that has affected the user’s weight.
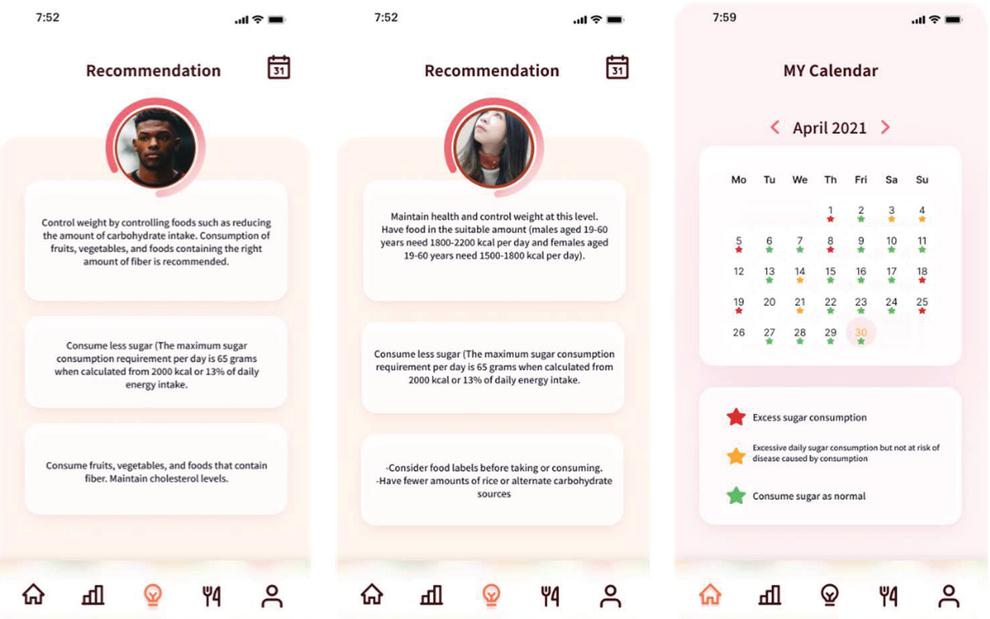
Figure 10 Recommendation results page.
When users press the menu icon, a guide will pop up in the form of an individual recommendation window, as shown in Figure 10. The calendar page shows users’ total monthly consumption results. A star icon appears in different colors to indicate on which days the user’s consumption was or not successful.
4.2 Mobile Application Evaluation
An assessment of user satisfaction was designed to prove the usability of the proposed application. Assessment criteria were measured using the aforementioned Likert scale. The user satisfaction results for all samples are presented in Table 7. Furthermore, The evaluation results for efficiency and user satisfaction among a sample of 140 Thai adolescents are reported in Table 7.
Table 7 User satisfaction results for function and personalization
| No. | Item | Mean | Assessment Criteria Level |
| Satisfaction: Function | |||
| 1 | The application overall has functions that can be easily used | 4.31 | Very High |
| 2 | The application is useful in daily life | 4.27 | Very High |
| 3 | The classification of the content is clear and appropriate | 4.24 | Very High |
| 4 | The application has a background and menus that are appealing to use | 4.10 | High |
| 5 | The format of the information presented in the application is easy to read and use | 4.25 | Very High |
| 6 | The basic functions of the application are easy to use | 4.32 | Very High |
| Average | 4.25 | Very High | |
| Satisfaction: Personalization | |||
| 7 | Information and advice are presented according to users’ needs | 4.39 | Very High |
| 8 | Using the application’s personal recommendation function is easy and convenient | 4.33 | Very High |
| 9 | The personalized content presented by the application is easy to understand | 4.23 | Very High |
| 10 | This module is essential to maintaining your health | 4.26 | Very High |
| Average | 4.30 | Very High | |
4.2.1 User satisfaction with function and personalization
Table 7 shows that user satisfaction with both function and personalization was very high. Users were more satisfied by the personalization than the function of the mobile application. With regard to function-related satisfaction, the item measuring whether users thought the application’s basic functions were easy to use obtained the highest satisfaction score. With regard to personalization-related satisfaction, the presentation of information and advice achieved the highest satisfaction score.
4.2.2 Evaluation of degree of awareness
With regard to degree of awareness, users’ preferences regarding the three degrees of awareness described previously were investigated. The satisfaction results for these three degrees of awareness at different testing periods are shown in Table 8.
Table 8 Evaluation results for degree of awareness
| Percentage of | ||||
| Respondents | ||||
| Automatic | ||||
| Recommendation | ||||
| Level | ||||
| No. | Item | Zero | Partial | Full |
| 1 | If you want to go on a diet or control your sugar and carbohydrate consumption in the first three days, what kind of recommendations do you prefer? | 2 | 13 | 85 |
| 2 | If you want to go on a diet or control your sugar and carbohydrate consumption for a while (days four and five), what kind of recommendations do you prefer? | 7 | 7 | 86 |
| 3 | If you want to go on a diet or control your sugar and carbohydrate consumption for a while (days six and seven), what kind of recommendations do you prefer? | 4 | 11 | 86 |
As shown in Table 8, most users are satisfied with fully automatic recommendations for all three phases. In the first phase, 85% of users were satisfied with fully automatic recommendations, indicating that they were interested in receiving the appropriate recommendations as provided by the system without self-calculating. This evidence indicates that users may prefer to try using the appropriate recommendations as provided by the system, rather than working on recommendation creation themselves (whether partial or full participation). Fully automatic recommendations were also preferred in the other phases by 86% of all users. It can thus be concluded that the application can successfully engage users to follow the recommendations provided by the system. Consequently, the proposed mobile application is deemed suitable for the target group (Thai adolescents). In future work, we aim to apply the personalized recommendation application with other target groups.
4.3 Discussion and Future Work
In this study, 144 pre-referral rules were created, which may not be enough for users of various age groups. Therefore, in future work, we plan to use machine learning and context awareness to apply users’ data to precisely categorize people and lifestyles to create automatic recommendations. We will avoid having the user prepare the rules, as here, and will be as flexible as possible in responding to the user’s individual characteristics. The background and menus of the application require improvement to increase user satisfaction—a worthwhile endeavor for future work. However, improving the personalized content to be more understandable could be considered in future work. In addition, future studies should focus on expanding the use of the application to different age groups.
5 Conclusion
This study proposes a context-aware personalized recommendation mobile application for Thai adolescents to monitor their excessive sugar consumption and provide them with proper individualized recommendations. The proposed mobile application applies a multi-nutritional criteria decision model together with the context-awareness principle to provide individual recommendations based on the user’s personal, health, and lifestyle data. Experiments were conducted with 140 Thai adolescents aged between 15 to 25 years old. The mobile application was evaluated in terms of efficiency, user satisfaction, and degree of awareness. The results showed that the developed mobile application obtained very high user satisfaction with regard to both function and personalization. Fully automatic recommendations were the most preferred presentation style by the evaluation group of young users. In future work, testing should be extended to include other generation groups.
Appendix
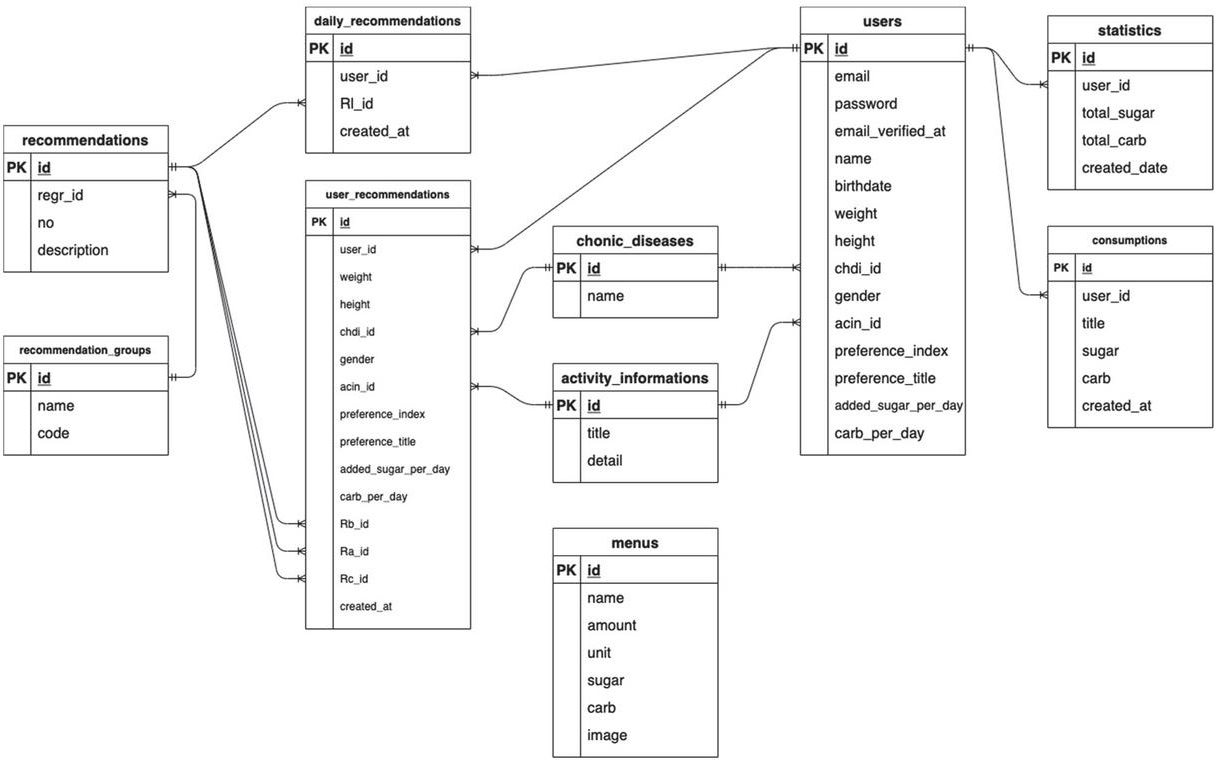
Figure 11 Entity relationship diagram for mobile application development representing all dataset links and data relationships in proposed application.
Acknowledgments
This research is supported by Mae Fah Luang University and Talent Mobility Project entitled “Mobile Application for Excessive Sugar Consumption Monitoring for Thai Teenager”. The publication is supported by the Capacity building and ExchaNge towards attaining Technological Research and modernizing Academic Learning-CENTRAL, which is funded by the Erasmus+ program (Project ID: 598914).
References
[1] W. Kriengsinyos, P. Chan, and M. S. V Amarra, “Consumption and sources of added sugar in Thailand: A review,” Asia Pacific Journal of Clinical Nutrition, vol. 27, no. 2. pp. 262–283, 2018. doi: 10.6133/apjcn.042017.08.
[2] J. M. Rippe and T. J. Angelopoulos, “Sugars, obesity, and cardiovascular disease: results from recent randomized control trials,” European Journal of Nutrition, vol. 55, pp. 45–53, Nov. 2016, doi: 10.1007/s00394-016-1257-2.
[3] K. Papier et al., “Consumption of sugar-sweetened beverages and type 2 diabetes incidence in Thai adults: Results from an 8-year prospective study,” Nutrition and Diabetes, vol. 7, no. 6, 2017, doi: 10.1038/nutd.2017.27.
[4] R. Clemens and Y. Papanikolaou, “Crystalizing global sugar policy: Public health promise or perception,” in Fructose, High Fructose Corn Syrup, Sucrose and Health, Springer New York, 2014, pp. 125–135. doi: 10.1007/978-1-4899-8077-9\_8.
[5] S. Phulkerd, N. Thongcharoenchupong, A. Chamratrithirong, R. Soottipong Gray, and P. Prasertsom, “Changes in population-level consumption of taxed and non-taxed sugar-sweetened beverages (Ssb) after implementation of ssb excise tax in Thailand: A prospective cohort study,” Nutrients, vol. 12, no. 11, pp. 1–15, Nov. 2020, doi: 10.3390/nu12113294.
[6] A. A. Abdellatif, A. Mohamed, C. F. Chiasserini, M. Tlili, and A. Erbad, “Edge computing for smart health: Context-aware approaches, opportunities, and challenges,” IEEE Network, vol. 33, no. 3, pp. 196–203, May 2019, doi: 10.1109/MNET.2019.1800083.
[7] M. C. Zanchim, V. R. Kirsten, and A. C. B. de Marchi, “Consumption of dietary intake markers by patients with diabetes assessed using a mobile application,” Ciencia e Saude Coletiva, vol. 23, no. 12, pp. 4199–4208, Dec. 2018, doi: 10.1590/1413-812320182312.01412017.
[8] I. Sutedja, R. Bahana, and I. B. K. Manuaba, “Foods Diary Mobile Application for Diabetics,” in 2020 International Conference on Information Management and Technology (ICIMTech), 2020, pp. 228–232. doi: 10.1109/ICIMTech50083.2020.9211125.
[9] R. Salari, S. R Niakan Kalhori, M. GhaziSaeedi, M. Jeddi, M. Nazari, and F. Fatehi, “Mobile-Based and Cloud-Based System for Self-management of People With Type 2 Diabetes: Development and Usability Evaluation,” Journal of Medical Internet Research, vol. 23, no. 6, p. e18167, Jun. 2021, doi: 10.2196/18167.
[10] V. Subramaniyaswamy et al., “An ontology-driven personalized food recommendation in IoT-based healthcare system,” Journal of Supercomputing, vol. 75, no. 6, pp. 3184–3216, Jun. 2019, doi: 10.1007/s11227-018-2331-8.
[11] N. Hamzeheinejad and H. P. @ Affal, “Mobile Food Consumption Monitoring Application,” Journal of Food Technology Research, vol. 3, no. 2, pp. 88–98, 2016, doi: 10.18488/journal.58/2016.3.2/58.2.88.98.
[12] R. Suwan and P. Temdee, “Lifestyle Classification for Recommendation of Excessive Sugar Consumption in Thai Teenagers,” in 2021 Joint 6th International Conference on Digital Arts, Media and Technology with 4th ECTI Northern Section Conference on Electrical, Electronics, Computer and Telecommunication Engineering, ECTI DAMT and NCON 2021, Mar. 2021, pp. 380–383. doi: 10.1109/ECTIDAMTNCON51128.2021.9425692.
[13] T. A. Dennis and L. J. O’Toole, “Mental health on the go: Effects of a gamified attention-bias modification mobile application in trait-anxious adults,” Clinical Psychological Science, vol. 2, no. 5, pp. 576–590, Dec. 2014, doi: 10.1177/2167702614522228.
[14] E. Toader, E. D. Mitrica, and G. Balan, “Mobile phone interventions in the healthcare of chronic diseases,” in In 2015 E-Health and Bioengineering Conference (EHB), 2015, pp. 1–4. doi: 10.1109/EHB.2015.7391417.
[15] J. Daly et al., “SleepCare: obstructive sleep apnoea screening using mobile health technology,” in Appropriate Healthcare Technologies for Low Resource Settings (AHT 2014), 2014, pp. 1–4. doi: 10.1049/cp.2014.0765.
[16] D. Cedeno-Moreno and M. Vargas-Lombardo, “Mobile Applications for Diabetes Self-Care and Approach to Machine Learning,” International journal of online and biomedical engineering, vol. 16, no. 8, pp. 25–38, 2020, doi: 10.3991/ijoe.v16i08.13591.
[17] Y. Zou, R. S. H. Istepanian, X. Wang, and T. Geake, “Design and Implementation of a Mobile Diabetes Management System,” Journal of Mobile Multimedia, vol. 1, no. 4, pp. 273–284, 2006.
[18] U. Gogate, M. Marathe, J. Mourya, and N. Mohan, “Android Based Health Monitoring System for Cardiac Patients,” International Research Journal of Engineering and Technology, vol. 4, no. 04, pp. 1628–1634, 2017, [Online]. Available: www.irjet.net
[19] N. Pandria, D. Spachos, and P. D. Bamidis, “The Future of Mobile Health ADHD Applications,” in 2015 International Conference on Interactive Mobile Communication Technologies and Learning (IMCL), 2015, vol. 61, no. 1, pp. 279–282. doi: 10.1109/IMCTL.2015.7359603.
[20] R. Ferrero, M. Rebaudengo, and F. Rosique, “Personal Assistance and Monitoring Devices Applications,” Advances in Human-Computer Interaction. 2019. doi: 10.1155/2019/8916796.
[21] A. F. C. Garces and J. P. O. Lojo, “Developing an Offline Mobile Application with Health Condition Care and First Aid Instruction for Appropriateness of Medical Treatment,” in 2019 IEEE Integrated STEM Education Conference (ISEC), 2019, pp. 13–14. doi: 10.1109/ISECon.2019.8882013.
[22] L. M. Y. Chung, S. S. M. Fong, and Q. P. S. Law, “Younger adults are more likely to increase fruit and vegetable consumption and decrease sugar intake with the application of dietary monitoring,” Nutrients, vol. 13, no. 2, pp. 1–12, Feb. 2021, doi: 10.3390/nu13020333.
[23] N. Rešèiè, E. Valenèiè, E. Mlinariè, B. K. Seljak, and M. Luštrek, “Mobile nutrition monitoring for well-being,” in UbiComp/ISWC 2019 – Adjunct Proceedings of the 2019 ACM International Joint Conference on Pervasive and Ubiquitous Computing and Proceedings of the 2019 ACM International Symposium on Wearable Computers, Sep. 2019, pp. 1194–1197. doi: 10.1145/3341162.3347076.
[24] G. D. Abowd, A. K. Dey, P. J. Brown, N. Davies, M. Smith, and P. Steggles, “Towards a Better Understanding of Context and Context-Awareness,” in International symposium on handheld and ubiquitous computing, 1999, pp. 304–307. doi: 10.1007/3-540-48157-5\_29.
[25] F. Adelstein, S. K. S. Gupta, G. G. Richard III, and L. Schwiebert, “Fundamentals of mobile and pervasive computing,” vol. 1, McGraw-Hill, 2005.
[26] N. M. Villegas, C. Sánchez, J. Díaz-Cely, and G. Tamura, “Characterizing context-aware recommender systems: A systematic literature review,” Knowledge-Based Systems, vol. 140, pp. 173–200, Jan. 2018, doi: 10.1016/j.knosys.2017.11.003.
[27] M. Mohammadian, Y. Forghani, and M. N. Torshiz, “An initialization method to improve the training time of matrix factorization algorithm for fast recommendation,” Soft Computing, vol. 25, no. 5, pp. 3975–3987, Mar. 2021, doi: 10.1007/s00500-020-05419-0.
[28] G. Agapito et al., “DIETOS: A dietary recommender system for chronic diseases monitoring and management,” Computer Methods and Programs in Biomedicine, vol. 153, pp. 93–104, Jan. 2018, doi: 10.1016/j.cmpb.2017.10.014.
[29] A. Sharma and R. Kumar, “A constrained framework for context-aware remote E-healthcare (CARE) services,” Transactions on Emerging Telecommunications Technologies. pp. 1–19, 2019. doi: 10.1002/ett.3649.
[30] M. Quinde, J. C. Augusto, N. Khan, and A. van Wyk, “ADAPT: Approach to Develop context-Aware solutions for Personalised asthma managemenT,” Journal of Biomedical Informatics, vol. 111, Nov. 2020, doi: 10.1016/j.jbi.2020.103586.
[31] M. Esposito, A. Minutolo, R. Megna, M. Forastiere, M. Magliulo, and G. de Pietro, “A smart mobile, self-configuring, context-aware architecture for personal health monitoring,” Engineering Applications of Artificial Intelligence, vol. 67, pp. 136–156, Jan. 2018, doi: 10.1016/j.engappai.2017.09.019.
[32] J. Hu, W. Liang, O. Hosam, M. Y. Hsieh, and X. Su, “5GSS: a framework for 5G-secure-smart healthcare monitoring,” Connection Science, 2021, doi: 10.1080/09540091.2021.1977243.
[33] M. M. Aborokbah, S. Al-Mutairi, A. K. Sangaiah, and O. W. Samuel, “Adaptive context aware decision computing paradigm for intensive health care delivery in smart cities—A case analysis,” Sustainable Cities and Society, vol. 41, pp. 919–924, Aug. 2018, doi: 10.1016/j.scs.2017.09.004.
[34] M. A. Serhani, M. el Menshawy, and A. Benharref, “SME2EM: Smart mobile end-to-end monitoring architecture for life-long diseases,” Computers in Biology and Medicine, vol. 68, pp. 137–154, Jan. 2016, doi: 10.1016/j.compbiomed.2015.11.009.
[35] H. Mshali, T. Lemlouma, and D. Magoni, “Adaptive monitoring system for e-health smart homes,” Pervasive and Mobile Computing, vol. 43, pp. 1–19, Jan. 2018, doi: 10.1016/j.pmcj.2017.11.001.
[36] F. Muheidat, L. Tawalbeh, and H. Tyrer, “Context-Aware, Accurate, and Real Time Fall Detection System for Elderly People,” in Proceedings – 12th IEEE International Conference on Semantic Computing, Apr. 2018, pp. 329–333. doi: 10.1109/ICSC.2018.00068.
[37] B. L. Sujaya and R. S. Bhaskar, “A Modelling of Context-Aware Elderly Healthcare Eco-System-(CA-EHS) Using Signal Analysis and Machine Learning Approach,” Wireless Personal Communications, vol. 119, no. 3, pp. 2501–2516, Aug. 2021, doi: 10.1007/s11277-021-08341-2.
[38] P. Temdee and R. Prasad, Context-Aware Communication and Computing: Applications for Smart Environment. Cham: Springer International Publishing, 2018.
[39] L. Qin, X. Xu, and J. Li, “A real-time professional content recommendation system for healthcare providers’ knowledge acquisition,” in Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics), 2018, pp. 367–371. doi: 10.1007/978-3-319-94301-5\_31.
[40] I. Paramonov, A. Vasilyev, and P. G. Demidov, “Recommendation Service for Smart Space-based Personalized Healthcare System,” in 2016 19th Conference of Open Innovations Association (FRUCT), 2016, pp. 182–188. doi: 10.23919/FRUCT.2016.7892199.
[41] D. Chen, D. Jin, T. T. Goh, N. Li, and L. Wei, “Context-Awareness Based Personalized Recommendation of Anti-Hypertension Drugs,” Journal of Medical Systems, vol. 40, no. 9, pp. 1–10, Sep. 2016, doi: 10.1007/s10916-016-0560-z.
[42] S. Chaising, R. Prasad, and P. Temdee, “Personalized Recommendation Method for Preventing Elderly People from Cardiovascular Disease Complication Using Integrated Objective Distance,” Wireless Personal Communications, vol. 117, no. 1, pp. 215–233, Mar. 2021, doi: 10.1007/s11277-019-06639-w.
[43] N. Rachata, W. Rueangsirarak, C. Kamyod, and P. Temdee, “Fuzzy Near Compactness Based Personalized Recommendation for Preventing Patients with Type 2 Diabetes Mellitus and Hypertension from Cardiovascular Complication,” Wireless Personal Communications, vol. 115, no. 4, pp. 3073–3097, Dec. 2020, doi: 10.1007/s11277-020-07532-7.
[44] J. C. C. Tseng et al., “An Interactive Healthcare System with Personalized Diet and Exercise Guideline Recommendation,” in 2015 Conference on Technologies and Applications of Artificial Intelligence (TAAI), 2015, pp. 525–532. doi: 10.1109/TAAI.2015.7407106.
[45] J. Ni, L. Muhlstein, and J. McAuley, “Modeling heart rate and activity data for personalized fitness recommendation,” in The Web Conference 2019 - Proceedings of the World Wide Web Conference, WWW 2019, May 2019, pp. 1343–1353. doi: 10.1145/3308558.3313643.
[46] S. Dharia et al., “PRO-Fit: Exercise with friends,” in 2016 IEEE/ACM International Conference on Advances in Social Networks Analysis and Mining (ASONAM), 2016, pp. 1430–1433. doi: 10.1109/ASONAM.2016.7752437.
[47] B. Chekima, A. I. Oswald, S. A. W. S. K. Wafa, and K. Chekima, “Narrowing the gap: Factors driving organic food consumption,” Journal of Cleaner Production, vol. 166, pp. 1438–1447, Nov. 2017, doi: 10.1016/j.jclepro.2017.08.086.
[48] M. G. Thorpe, C. M. Milte, D. Crawford, and S. A. McNaughton, “A revised Australian dietary guideline index and its association with key sociodemographic factors, health behaviors and body mass index in peri-retirement aged adults,” Nutrients, vol. 8, no. 3, pp. 1–12, Mar. 2016, doi: 10.3390/nu8030160.
[49] World Health Organization, Guideline: Sugars intake for adults and children. 2015.
[50] C. Darviri et al., “The Healthy Lifestyle and Personal Control Questionnaire (HLPCQ): A novel tool for assessing self-empowerment through a constellation of daily activities,” BMC Public Health, vol. 14, no. 1, Sep. 2014, doi: 10.1186/1471-2458-14-995.
[51] P. Temdee and R. Prasad, “Context and Its Awareness,” in Context-Aware Communication and Computing: Applications for Smart Environment, Springer, Cham, 2018, pp. 15–31. doi: 10.1007/978-3-319-59035-6\_2.
[52] B. H. C. Cheng et al., “SEAMS 2009: Software Engineering forAdaptive and Self-Managing Systems,” in 2009 31st International Conference on Software Engineering – Companion Volume, 2009, pp. 463–464. doi: 10.1109/ICSE-COMPANION.2009.5071063.
[53] S. Hallsteinsen et al., “A development framework and methodology for self-adapting applications in ubiquitous computing environments,” Journal of Systems and Software, vol. 85, no. 12, pp. 2840–2859, Dec. 2012, doi: 10.1016/j.jss.2012.07.052.
[54] B. Y. Lim and A. K. Dey, “Assessing Demand for Intelligibility in Context-Aware Applications,” in In Proceedings of the 11th international conference on Ubiquitous computing, 2009, pp. 195–204. doi: 10.1145/1620545.1620576.
[55] M. Mori, “A Software Lifecycle Process for Context-Aware AdaptiveSystems,” in In Proceedings of the 19th ACM SIGSOFT Symposium and the 13th European conference on Foundations of Software Engineering, 2011, pp. 412–415. doi: 10.1145/2025113.2025177.
[56] P. P. Sirichakwal, K. Sranacharoenpong, and K. Tontisirin, “Food based dietary guidelines (FBDGs) development and promotion in Thailand,” Asia Pacific Journal of Clinical Nutrition, vol. 20, no. 3, pp. 477–483, 2011.
[57] A. Misra et al., “Consensus dietary guidelines for healthy living and prevention of obesity, the metabolic syndrome, diabetes, and related disorders in Asian Indians,” Diabetes Technology and Therapeutics, vol. 13, no. 6, pp. 683–694, Jun. 2011, doi: 10.1089/dia.2010.0198.
[58] A. B. Peinado, M. A. Rojo-Tirado, and P. J. Benito, “Sugar and physical exercise; the importance of sugar for athletes,” in Nutricion hospitalaria: organo oficial de la Sociedad Espanola de Nutricion Parenteral y Enteral (NUTR HOSP), 2013, pp. 48–56. doi: 10.3305/nh.2013.28.sup4.6796.
[59] National Heart Lung and Blood Institute., “Your Guide to Lowering Your Cholesterol With TLC,” Bethesda, MD: US Department of Health and Human Service. Bethesda, MD: US Department of Health and Human Service., 2005.
[60] V. Misra, A. K. Shrivastava, S. P. Shukla, and M. I. Ansari, “Effect of sugar intake towards human health,” Saudi Journal of Medicine, vol. 1, no. 2, pp. 29–36, 2016, doi: 10.21276/sjm.2016.1.2.2.
[61] N. F. Hamd, N. N. Naing, R. Abdul Jalil, and S. Yamamoto, “Development and Validation of the Beverages and Snacks Questionnaire for Malaysian Schoolchildren (BSQ-C),” Environment-Behaviour Proceedings Journal, vol. 4, no. 12, pp. 3–9, Dec. 2019, doi: 10.21834/e-bpj.v4i12.1909.
[62] M. Grossman, “Food labels and labeling in the United States,” European Food and Feed Law Review, 2015.
Biographies

Rodjana Suwan received the bachelor’s degree in B.S. (ANIMATION) from Chiang Mai University in 2013. She is currently working as a computer technician and studying at the School of Information Technology, Mae Fah Luang University, Chiang Rai, Thailand. Her research interests include mobile application, artificial intelligence, and machine learning.

Punnarumol Temdee received B.Eng. in Electronic and Telecommunication Engineering, M. Eng in Electrical Engineering, and Ph.D. in Electrical and Computer Engineering from King Mongkut’s University of Technology Thonburi. She is currently a lecturer at School of Information Technology, Mae Fah Luang University, Chiang Rai, Thailand. Her research interests are social network analysis, artificial intelligence, software agent, context-aware computing, and ubiquitous computing.

Ramjee Prasad is currently a Professor of Future Technologies for Business Ecosystem Innovation (FT4BI) in the Department of Business Development and Technology, Aarhus University, Denmark. He is the Founder President of the CTIF Global Capsule (CGC). He is also the Founder Chairman of the Global ICT Standardisation Forum for India, established in 2009. He has published over 1000 technical papers, more than 15 patents, contributed to several books and has authored, co-authored, and edited over 30 books.
Journal of Mobile Multimedia, Vol. 18_6, 1879–1912.
doi: 10.13052/jmm1550-4646.18618
© 2022 River Publishers