Knowledge and Awareness of COVID-19 in Uttar Pradesh: An Exploratory Data Analysis
Prayas Sharma1,*, Nitesh Kumar Adichwal2 and Ashish Kumar Singh3
1Indian Institute of Management Sirmaur, Sirmaur, Himachal Pradesh, India
2University of petroleum & Energy Studies, Dehradun, Uttarakhand, India
3Department of Management Studies, Raj Kumar Goel Institute of Technology, Ghaziabad, India
E-mail: prayassharma02@gmail.com
*Corresponding Author
Received 21 February 2022; Accepted 30 May 2022; Publication 27 July 2022
Abstract
Corona viruses, commonly called COVID-19, are a large family of viruses that can cause diseases ranging from the common cold to Severe Acute Respiratory Syndrome (SARS). Worldwide Covid-19 is affecting 210 countries and territories around the world and two international conveyances. As of 2 June 2020, there are 6,408,869 confirmed 2,935,368 recovered and 378,317 deaths cases has been reported in world of Coronavirus diseases, India is not untouched from this situation. Currently, it has reported infected 190,535 and 5,394 death cases due to COVID-19 in India. (https://covid19.who.int/region/searo/country/in). The COVID-19 pandemic was first confirmed in the Indian state of Uttar Pradesh on 4 March 2020, with the first positive case in Ghaziabad. As of 1 June 2020, the state has 8361 confirmed cases, resulting in 222 deaths and 5030 recoveries. The situation is getting worst day by day as COVID-19 outbreaks and patients are increasing by every minute and become the most important issue for the whole world and So accessing knowledge and awareness among the people is very important. The present study using the exploratory data analysis we tried to demonstrate the knowledge and awareness of individuals about the COVID-19 pandemic in Uttar Pradesh, the most populous state of India. The findings of the present study can be utilized by the researchers and policy makers to handle this worst situation.
Keywords: Awareness, frequency distribution, data analysis, policy making, COVID-19.
1 Introduction
A novel human coronavirus, named as severe respiratory syndrome coronavirus subsequently named as SARS-CoV-2 was first reported in Wuhan, China, in December 2019 (Holshue et al., 2020; Sohrabi et al., 2020). Published literature can trace the beginning of symptomatic individuals back to the beginning of December 2019. In a meeting on January 30, 2020, as per the International Health Regulations (IHR, 2005) emergency committee, the outbreak of Novel coronavirus (2019-nCoV) was declared by the WHO a Public Health Emergency of International Concern (PHEIC) as it had spread to 18 countries with four countries reporting human-to-human transmission. On February 11, 2020, the WHO Director-General, Dr. Tedros Adhanom Ghebreyesus, announced that the disease caused by this new CoV was a “COVID-19,” which is the acronym of “coronavirus disease 2019”. This new virus seems to be very contagious and has quickly spread globally. COVID-19 is spreading rapidly throughout the world; approximately all developed and developing countries and nations (Amirhossein Takian and Kazempour-Ardebili, 2020; Holshue et al., 2020; Sohrabi et al., 2020; van Doremalen et al., 2020a). On March 11, as the number of COVID-19 cases outside China has increased 13 times and the number of countries involved has tripled with more than 118,000 cases in 114 countries and over 4,000 deaths, WHO declared the COVID-19 outbreak as a pandemic.
The first case of COVID-19 was reported in India on 30th January 2020 with origin from China (PIB, 2020). It spreads to the maximum districts of the country. This has resulted in lockdown in many nations worldwide. On 24 March, the Government of India ordered a nationwide lockdown for 21 days, limiting movement of the entire 1.3 billion population of India as a preventive measure against the 2020 coronavirus pandemic in India. It was ordered after a fourteen-hour voluntary public curfew on 22 March, followed by enforcement of a series of regulations in the country’s COVID-19 affected regions. The lockdown was placed when the number of confirmed positive coronavirus cases in India was approximately 500. This lockdown enforces restrictions and self-quarantine measures. Lockdown was extended the nationwide till 3 May, with a conditional relaxation promised after 20 April for the regions where the spread had been contained by then.
As on 27th April 2020, the total cases reported in India are 29435 with 6869 recoveries and 934 deaths (Covid-19.in, 2020). Hospital isolation of all confirmed cases, tracing and home quarantine of the contacts is ongoing. However, the rate of infection in India is lower as compared to other countries. Common signs and symptoms of COVID-19 infection include symptoms of severe respiratory disorders such as fever, coughing and shortness of breath. The virus that causes COVID-19 is mainly transmitted through droplets generated when an infected person coughs, sneezes, or exhales. These droplets are too heavy to hang in the air, and quickly fall on floors or surfaces. The average incubation period is 5–6 days with the longest incubation period of 14 days. In severe cases, covid-19 can cause pneumonia, acute respiratory syndrome, kidney failure, and even death. The clinical signs and symptoms reported in the majority of cases are fever, with some cases having difficulty breathing, and X-rays show extensive pneumonia infiltrates in both lungs (Holshue et al., 2020; Perlman, 2020). The clinical symptoms of severe and critical patients with covid-19 are likely similar with the clinical symptoms of SARS and MERS (Wang et al., 2020b). Preventive measures for COVID-19 include maintaining social distancing, washing hands frequently, avoiding touching the mouth, nose, and face (WHO, 2020).
Knowledge and awareness during the people of India played an important role to save them from COVID-19. Even the health ministries mentioned that awareness can be one of the important thing to fight against COVID-19 and remain safe. Authors like Singh et al. (2020), Sharma et al. (2020) studies the importance of knowledge and awareness among the Indian citizens. They recommended that urban societies were less affected both in terms of numbers and severity as compare to the rural because of their education level and awareness. It is fact that testing in the rural area was limited and therefore numbers may reflect the against the analysis and recommendation of the literature. Uttar Pradesh is the most populous state of India holds more than 166 million people, therefore we focused on the state Uttar Pradesh for our study.
Because of the heterogeneity in populations, the estimates show variation with respect to certain background characteristics like variation among age group, caste, marital status etc. Therefore, in order to get complete picture of the scenario, it is important to study these estimates with respect to their background characteristics. There are few studies, which have discussed about knowledge, perception, attitude and risk behaviour of COVID-19. This study attempts to know how the knowledge and awareness changes among people of Uttar Pradesh with respect to certain background characteristics and that in conformity with gender wise variation. It also tries to know the risk behaviour about COVID-19. With aforesaid background we restricted ourselves to following two objectives:
• To assess the knowledge and Awareness among people living in Uttar Pradesh.
• To access the risk behaviour about COVID-19 among peoples having different occupations.
2 Data and Methods
Our study was cross-sectional, carried out by a convenience non probability sampling technique in India. A semi-structured questionnaire was developed in very easy understandable English by using Google form. The questionnaire was disseminated through WhatsApp, e-mails and through social media platforms to the known contacts. The participants showed enough interest to give their response and also forwarded it to their contacts, which resulted to get the response from all over the states. Participants possessing smart phones & internet have participated in the study, which is very common in nowadays society. Participants above to 15 years and comfortable with English and shown their willingness have given their inputs. Total we received 533 responses, but some were filled incomplete, so we eliminated them. Finally, we analysed on 448 responses to draw our results. The socio-demographic profile of respondents was accessed by questionnaire, which includes gender, age, education, place of residence, domicile, marital status, etc.
The questionnaire given to respondents contained separate section to know how they commute and interact to peoples, trusted source of information, 2 questions to evaluate the threat level of virus, one dichotomous question for awareness about health facility, 6 questions to estimate awareness level of corona virus in society, 11 questions for symptoms, 12 questions for perception about prevention from corona virus. The process of data collection was held during 11th, April 2020 to 28th, April 2020.
3 Definition of Variables
This section describes the definition of the variables constructed and used in the analysis.
• Age
Age has been classified into four groups – 15–25, 26–35, 36–45, 46–55.
• Place of Residence
Place of residence has divided in to two categories Rural and Urban.
• Marital Status
Marital status has been classified in to four categories Single/Never married, Divorce/Separated, Widow(er)
• Qualification
Qualification has been divided in to five parts UG, PG, Ph.D., Other, Diploma.
• Occupation
Occupation has been divided in to ten categories Salaried Government, Salaried Private, Business/Self Employed, Doctor/Health care provider, Agriculture worker, working for non profit/ government organisation, student, House wife/Home maker, Retired and others.
• COVID-19 Related Knowledge
The knowledge of COVID-19 has been judge using the following questions.
Corona can be caused by virus, can spread from one person to another, It can be prevented, It is same as common cold, Occurs at certain period of the year, COVID-19 symptoms are worse among Diabetic.
• Knowledge about COVID-19 symptoms
The knowledge regarding COVID-19 symptoms has been checked using the following symptoms
Headache, Sore Throat, Vomiting, Persistent Cough, Running Nose, Sneezing, Muscle Ache, Abdominal Pain, Fever, Diarrhoea, Feeling Tired.
• Source of information: has been classified into the following groups
Official Government Website, Office Colleagues, Doctor/Nurse, Neighbour, Radio, Newspaper, Facebook/Twitter/Instagram, Family member, WhatsApp, Television
Table 1 Percentage distribution of population by their socio economic characteristics
| Males | Females | Total | ||||
| Background Characteristics | n | % | n | % | n | % |
| Age Group | ||||||
| 15–25 | 136 | 51.7 | 99 | 53.5 | 235 | 52.5 |
| 26–35 | 65 | 24.7 | 57 | 30.8 | 122 | 27.2 |
| 36–45 | 39 | 14.8 | 17 | 9.2 | 56 | 12.5 |
| 46–55 | 23 | 8.7 | 12 | 6.5 | 35 | 7.8 |
| Place of Residence | ||||||
| Rural | 46 | 17.5 | 39 | 21.1 | 85 | 19.0 |
| Urban | 217 | 82.5 | 146 | 78.9 | 363 | 81.0 |
| Marital Status | ||||||
| Single/Never Married | 169 | 64.3 | 126 | 68.1 | 295 | 65.8 |
| Married | 92 | 35.0 | 56 | 30.3 | 148 | 33.0 |
| Divorced/Seprated | 1 | 0.4 | 2 | 1.1 | 3 | 0.7 |
| Widow(er) | 1 | 0.4 | 1 | 0.5 | 2 | 0.4 |
| Qualificaiton | ||||||
| UG | 103 | 39.2 | 53 | 28.6 | 156 | 34.8 |
| PG | 117 | 44.5 | 96 | 51.9 | 213 | 47.5 |
| Ph.D | 26 | 9.9 | 21 | 11.4 | 47 | 10.5 |
| Other | 15 | 5.7 | 13 | 7.0 | 28 | 6.2 |
| Diploma | 2 | 0.8 | 2 | 1.1 | 4 | 0.9 |
| Occupation | ||||||
| Salaried Government | 41 | 15.6 | 12 | 6.5 | 53 | 11.8 |
| Salaried Private | 70 | 26.6 | 49 | 26.5 | 119 | 26.6 |
| Business/Self Employed | 20 | 7.6 | 2 | 1.1 | 22 | 4.9 |
| Doctor/Health Care Provider | NA | NA | 1 | 0.5 | 1 | 0.2 |
| Agriculture Worker | NA | NA | 1 | 0.5 | 1 | 0.2 |
| Working for Non Profit/Government Organisation | NA | NA | 2 | 1.1 | 2 | 0.4 |
| Student | 117 | 44.5 | 100 | 54.1 | 217 | 48.4 |
| House Wife/Home Maker | 1 | 0.4 | 14 | 7.6 | 15 | 3.3 |
| Retired | 4 | 1.5 | 1 | 0.5 | 5 | 1.1 |
| Others | 10 | 3.8 | 3 | 1.6 | 13 | 2.9 |
| NA not applicable. | ||||||
4 Results and Findings
Distribution of Population by Their Socio Economic Characteristics
Table 1 reveals the percent distribution of population by their socio economic characteristics. From the table it is clear that the major proportion of people (Males and Females), who have actively participated in the survey are lying between the age-group 15–24 and 26–35. However, the percentage of Females participation is slightly higher as compared with the Males for both the age-group. Most of the people are from Urban area. In terms of Marital status most of the people are either married or single.
The percentage of divorced/separated or widow/widower is very low. Major part of people (Males & Female both) are Graduate or Post Graduate. The participation of Ph.D., others or Diploma people is low compared with Graduate or Post Graduate people. In terms of Occupation major part of peoples are students followed by Salaried Private, Salaried Government Employee and Business/Self Employed.
Knowledge Regarding COIVD-19
Table 2 represents the knowledge of COVID-19 in UP. To access the knowledge of COVID-19 questions regarding cause of corona virus, it can be spread from one person to another, whether it can be prevented or not, Symptoms, whether it is periodic and the effect among Diabetic patients have been asked from the 448 respondents. From Table 2 it can be observed that out of 448 respondents 422 (94.2% of total respondent) respondent agreed that it is cause by virus. 98.4% of people are responding that it can be spread from one person to another. 77.9% people think that it can be prevented. Around 58.9% of people state that COVID-19 symptoms are worse among Diabetic.
Table 2 Knowledge about COVID-19
| Yes | No | Don’t Know | ||||
| Variables | n | % | n | % | n | % |
| Corona can be caused by virus | 422 | 94.2 | 14 | 3.1 | 12 | 2.7 |
| Can spread from one person to another | 441 | 98.4 | 1 | 0.2 | 6 | 1.3 |
| It can be prevented | 349 | 77.9 | 42 | 9.4 | 57 | 12.7 |
| It is same as common cold | 128 | 28.6 | 281 | 62.7 | 39 | 8.7 |
| Occurs at certain period of the year | 53 | 11.8 | 283 | 63.2 | 112 | 25 |
| COVID-19 symptoms are worse among Diabetic | 264 | 58.9 | 65 | 14.5 | 119 | 26.6 |
It may due to low immune systems of diabetic patients. On the other hand, 14.55 of people thinks that COVID-19 symptoms are not worse among Diabetic patients and around 25% states that they don’t know whether COVID-19 symptoms are worse or not among Diabetic patient which reflect the misconception among the people. Only 28.6% respondents state that the symptoms of COVID-19 is same as common cold, while 62.7% people states that the symptoms of COVID-19 is not same as common cold and 8.7% people don’t know whether the symptoms of COVID-19 is same as common cold or not. Around 11.8% people think that COVID-19 occurs at certain period of the year. Which reflect the misconception about COVID-19 among the people. Summarising to these result it is observed that most of the people are aware the corona is caused by virus, it can be spread from one person to another and about the prevention. On the other hand, many people also have misconception regarding COVID-19 as they think that it occurs at a certain period of the year, symptoms are not worse among diabetic patient and symptoms is not same as common cold.
Table 3 Knowledge about COVID-19 symptoms
| Common Coronavirus Symptoms | Yes % | No % |
| Headache | 61.2 | 38.8 |
| Sore Throat | 86.6 | 13.4 |
| Vomiting | 23.4 | 76.6 |
| Persistent Cough | 87.1 | 12.9 |
| Running Nose | 70.3 | 29.7 |
| Sneezing | 79.5 | 20.5 |
| Muscle Ache | 47.1 | 52.9 |
| Abdominal Pain | 27.2 | 72.8 |
| Fever | 98.4 | 1.6 |
| Diarrhea | 29.2 | 70.8 |
| Feeling Tired | 75.2 | 24.8 |
Knowledge regarding COVID-19 Symptoms
To access the knowledge regarding common symptoms of COVID-19 responses have been collected from 448 respondents. The result of the response is represented in Table 3. From Table 3, it is observed that only 61.2% of people think that Headache is common coronavirus symptoms. 86.6% people think that sore throat is the common symptoms. 23.4% people thinks that Vomiting is a common symptom. 87.1% people think persistent coughs as common symptoms, 70.3% thinks that running nose is a common symptom, 79.5% people think that sneezing is a common symptom, 47.1% thinks that muscle ache is a common symptom, 27.2% people state that Abdominal pain is a common symptom, 98.4% people thinks Fever is a common symptom, 29.2% people thinks Diarrhoea as a common symptom, 75.2% thinks that Feeling tired is a common symptom. Concluding to these result, it is observed that major part of the population thinks that fever is the main common coronavirus symptoms followed by persistent cough, sore throat, Sneezing, feeling tired, running nose and headache.
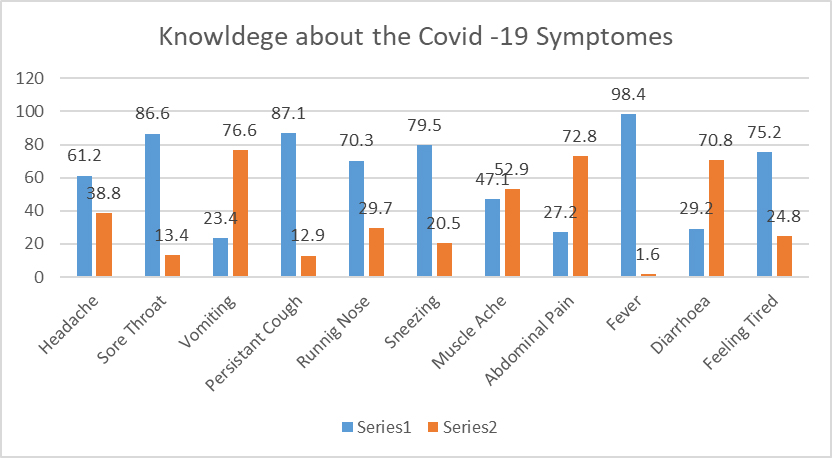
On the other hand, people also have some misconception regarding common coronavirus symptoms as they think that Muscle ache, Diarrhoea, Abdominal pain, vomiting are also a coronavirus symptom.
Table 4 Source of information
| Source | n | % |
| Official Government Website | 269 | 60.00 |
| Office Colleagues | 29 | 6.50 |
| Doctor/Nurse | 72 | 16.10 |
| Neighbor | 27 | 6.00 |
| Radio | 42 | 9.40 |
| Newspaper | 205 | 45.80 |
| Facebook/Twitter/Instagram | 85 | 19.00 |
| Family Member | 377 | 84.20 |
| 73 | 16.30 | |
| Television | 305 | 68.10 |
Source of Information
The question regarding the source of information about COVID-19 have been asked from the 448 respondent of UP. The response so obtained is present in Table 3. From Table 4 it is clear that the most of the people are getting information about COVID-19 from Family members (84.2%) followed by Television (68.1%), official government website (60%) and Newspaper (45.8%) as the percentage of getting information through these sources are higher as compared to rest sources.
Around 6.5% of people are getting information through office colleagues. 16.1% people are getting information from Doctor/Nurse. 6% of people are getting information through Neighbours. 9.4% of people are getting information from Radio. 19% of people are getting information through Facebook/Twitter/Instagram. 16.3% are getting information through Whatsapp.
Awareness
Table 5 reveals the awareness of COVID-19 among the people of UP. To access the awareness, the opinion of people was asked regarding, if someone develops symptoms of COVID-19, they should be quarantine and treated in the hospital, quarantine and sent home, they should be socially restricted to prevent cross infection, they should rapidly access to counselling services. The responses were collected in likert scale between 1 to 5. Where 1 reflect strongly agree and 5 reflects strongly disagree.
Table 5 Awareness regarding COVID-19
| According to you, if someone develops symptoms of Coronavirus | Weighted Mean |
| They should be quarantined and treated in the hospital | 1.26 |
| Quarantine and sent home | 2.85 |
| They should be socially restricted to prevent cross infection | 1.41 |
| They should rapidly access to counselling services | 1.89 |
| According to you what are the possible prevention from Coronavirus | |
| Exercise and Yoga | 2.01 |
| Avoid face to face meeting with people | 1.23 |
| Avoid travelling by any medium | 1.4 |
| Wash hands and face with soap during certain period of time | 1.17 |
| Avoid going to market | 1.42 |
| Avoid morning walk | 1.67 |
| Avoid going to the office | 1.51 |
| Always wearing mask and sanitize hands while stepping out | 1.17 |
| Eating Ginger/Garlic/Hot Chillies pepper | 2.07 |
| Drinking warm water | 1.54 |
| Avoid going out in Cold weather | 1.94 |
| Social Distancing | 1.09 |
The people were asked to rate the various ways to prevent from COVID-19 such as Exercise and Yoga, avoid face to face meeting with people, avoid travelling by any medium, Wash hands and face with soap during certain period of time, avoid going to market, avoid morning walk, avoid going to the office, always wearing mask and sanitize hands while stepping out, Eating Ginger/Garlic/Hot Chillies pepper, drinking warm water, avoid going out in Cold weather and Social Distancing between 1 to 5. Where 1 reflect strongly agree and 5 reflects strongly disagree. The people were also asked to give their opinion about, who are in greater risk of getting infected by COVID-19 among Doctors and Nurses, Other Hospital Staffs, Children, Senior Citizen, Diabetics, Airline Crew, Other Airport Staff, Frequent Air Travelers, Train/Bus Drivers, Rickshaw Pullers, Hawkers, Person with pre-existing morbidity condition, Pregnant Women, Girls during menstrual Period, People who eat non veg food, who works in Bank, who drink Alcohol or Who consume Tobacco.
Table 5 exhibits that most of the people are agree to keep person quarantine and treated in hospital for a person who develops symptoms of coronavirus. People are also agreeing for socially restricting the people who develop a symptoms of coronavirus to prevent from cross infection. Few people are also agreeing towards rapidly accessing to counselling service for a person who develop a symptoms of coronavirus. Most of the people are neutral towards agreeing to quarantine and sent home to a person who develop a symptoms of coronavirus.
The knowledge regarding prevention from coronavirus were access by asking them to rate various ways of prevention between 1 to 5. The result reveals that most of the people are agreeing that by social distancing, always wearing mask and sanitize hands while stepping out, wash hands and face with soap during certain period of time are the possible prevention from coronavirus.
Peoples are also agreeing that avoiding face to face meeting with people, avoid travel from any medium, avoid going to market, avoid morning walk, avoid going to office, drinking warm water weather are the possible ways to prevent from coronavirus. Few peoples also agree that Exercise and Yoga, Eating Ginger/Garlic/Hot Chillies pepper, avoiding going out in cold are the possible ways to prevent from coronavirus as their weighted means are close to 2.
Table 6 People who are at greater risk of getting infected
| Percent % | |
| Doctors and Nurses | 95.3 |
| Other Hospital Staffs | 94.4 |
| Children | 72.8 |
| Senior Citizen | 95.8 |
| Diabetics | 82.4 |
| Airline Crew | 78.8 |
| Other Airport Staff | 76.6 |
| Frequent Air Travellers | 83.3 |
| Train/Bus Drivers | 79.7 |
| Rickshaw Pullers | 76.1 |
| Hawkers | 72.8 |
| Person with pre-existing morbidity condition | 76.1 |
| Pregnant Women | 60.9 |
| Women/Girls during menstrural Period | 31.5 |
| People who eat Non veg Food | 43.8 |
| Who works in Bank | 65.8 |
| Who drinks Alcohol | 39.1 |
| Who Consume Tobacco | 50.4 |
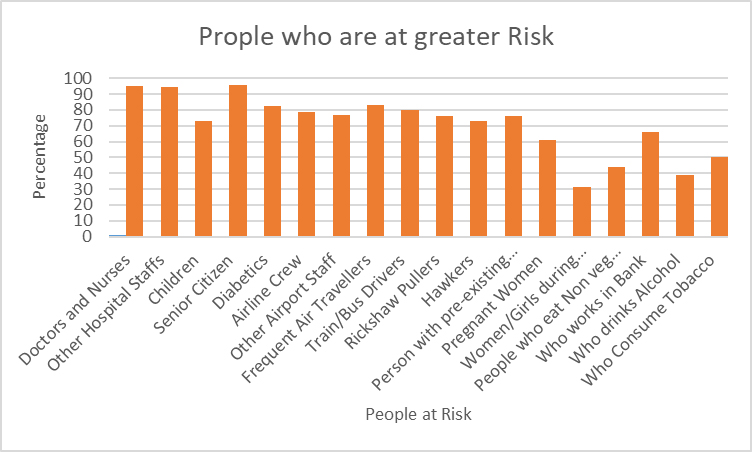
The questions were asked to access the opinion of the people about the people who are at greater risk of getting infected. From Table 6 it is clear that around 95.8% of people state that Senior citizen are at higher risk of getting infected by COVID-19 it may be due to having lower immunity problem at higher age. Around 95.3% of people state that Doctors are at higher risk of getting infected by COVID-19 followed by nurses and other hospital staffs because of the risk of transmission of disease from COVID-19 patients. 83.3% of people state that frequent air travelers are at higher risk of getting infection of COVID-19.
On the other hand, 78.8% people state that Airline Crew are at higher risk of getting infected followed by other airport staff (76.6%). 82.4% people state that Diabetics are at higher risk of getting infection of COVID-19. Around 79.7% of people state that train/Bus drivers are at higher risk of getting infected followed by rickshaw pullers (76.1%), Person with pre-existing morbidity condition (76.1%), Childen (72.8%), Hawkers (72.8%) and. Who works in bank (65.8%). Only 60.9% people agree that pregnant women are at higher risk of getting infection followed by who consume Tobacco (50.4%), people who eat non veg food (43.8%), Who drinks alcohol (39.1%) and Women/Girls during menstrual period (31.5%).
5 Conclusion
It has been observed that majority of people have knowledge about the COVID-19. On the other hands few peoples also have some misconception regarding COVID-19 and their symptoms as they think that it occurs at certain period of years, they think that Muscle ache, Diarrhoea, Abdominal pain, vomiting are also a coronavirus symptom. People knows about the symptoms of COVID-19. According to them, fever is the main common coronavirus symptoms followed by persistent cough, sore throat, Sneezing, feeling tired, running nose and headache.
Analysing the primary data collected from individuals we observed that family members are the main source of information about COVID-19 followed by Television, official government website and Newspaper. Less peoples are getting information from social media like facebook/twitter/Instagram and other sources such as Nurses/Doctors, Radio, Office colleagues etc.
Peoples are agreeing to keep person quarantine and treated in hospital for a person who develops symptoms of coronavirus. People are also agreeing for socially restricting the people who develop a symptoms of coronavirus to prevent from cross infection. Few people are also agreeing towards rapidly accessing to counselling service for a person who develop a symptoms of coronavirus. Most of the people are neutral towards agreeing to quarantine and sent home to a person who develop a symptoms of coronavirus.
People are agreeing that avoiding face to face meeting with people, avoid travel from any medium, avoid going to market, avoid morning walk, avoid going to office, drinking warm water weather are the possible ways to prevent from coronavirus. Few peoples also agree that Exercise and Yoga, Eating Ginger/Garlic/Hot Chillies pepper, avoiding going out in cold are the possible ways to prevent from COVID-19 infection.
People state that Senior citizen are at higher risk of getting infected by COVID-19 followed by Doctors, nurses and other hospital staffs. The risk is also high among frequent air traveler, Airline Crew and other airport staff, Diabetics, train/Bus drivers, rickshaw pullers, person with pre-existing morbidity condition, Childen, Hawkers and. Who works in bank. Pregnant women, people who consume Tobacco, people who eat non veg food, who drinks alcohol, and Women/Girls during menstrual period are also at risk but the risk among these peoples are comparatively low.
References
Anderson, R.M., Heesterbeek, H., Klinkenberg, D., Hollingsworth, T.D., (2020) How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet 395, 931–934.
Cucinotta, D., Vanelli, M., 2020. WHO declares COVID-19 a pandemic. Acta bio-medica: Atenei Parmensis 91, 157.
Dalziel, B.D., Kissler, S., Gog, J.R., Viboud, C., Bjørnstad, O.N., Metcalf, C.J.E., et al., (2018) Urbanization and humidity shape the intensity of influenza epidemics in U.S. cities. Science 362, 75–79.
Epstein, P.R. (2001) West Nile virus and the climate. J. Urban Health 78, 367–371.
Fitria, N., Setiawan, R., (2014) Identifikasi Karakteristik Lingkungan Permukiman Kumuh di Kelurahan Kapuk, Jakarta Barat. Jurnal Teknik ITS 3, C240–C244.
Holshue, M.L., DeBolt, C., Lindquist, S., Lofy, K.H., Wiesman, J., Bruce, H., et al., (2020) First case of 2019 novel coronavirus in the United States. N. Engl. J. Med.
Kementerian Kesehatan Republik Indonesia (2020) Pedoman Pencegahan dan Pengendalian Corona Virus Diaseases (COVID-19).
Li, Q., Guan, X.,Wu, P., Wang, X., Zhou, L., Tong, Y., et al., (2020) Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N. Engl. J. Med.
Ma Y, Zhao Y, Liu J, He X,Wang B, Fu S, et al. Effects of temperature variation and humidity on the mortality of COVID-19 in Wuhan. medRxiv 2020.
Mawarni, V., 2019. Kajian Evaluasi Kinerja Komite Sekolah di Provinsi DKI Jakarta.
Prosiding Seminar Nasional Pendidikan STKIP Kusuma Negara.
Perlman, S., (2020) Another decade, another coronavirus. Mass Medical Soc.
Poole, L., (2020) Seasonal Influences on the Spread of SARS-CoV-2 (COVID19), Causality, and Forecastabililty (3-15-2020). Causality, and Forecastabililty.
Sajadi,M.M., Habibzadeh, P., Vintzileos, A., Shokouhi, S., Miralles-Wilhelm, F.,Amoroso, A., (2020) Temperature and Latitude Analysis to Predict Potential Spread and Seasonality for COVID-19. Available at SSRN 3550308.
Sharma P, Singh AK, Agrawal B, & Sharma A. (2020): Correlation between weather and COVID-19 pandemic in India: An empirical investigation. Journal of Public Affairs. e2222. https://doi.org/10.1002/pa.2222.
Shi, P., Dong, Y., Yan, H., Li, X., Zhao, C., Liu, W., et al., (2020) The Impact of Temperature and Absolute Humidity on the Coronavirus Disease 2019 (COVID-19) Outbreak-Evidence from China. medRxiv.
Singh AK, Agrawal B, Sharma A & Sharma P. (2020) COVID-19: Assessment of knowledge and awareness in Indian society. Journal of Public Affairs; 20(4) e2354.
Sohrabi, C., Alsafi, Z., O’Neill, N., Khan, M., Kerwan, A., Al-Jabir, A., et al., (2020) World Health Organization declares global emergency: a review of the 2019 novel coronavirus (COVID-19). Int. J. Surg.
Surjadi, C., Surja, S.S., (2019) Kesehatan perkotaan di Indonesia: Penerbit Unika Atma Jaya Jakarta.
Tan, J., Mu, L., Huang, J., Yu, S., Chen, B., Yin, J., (2005) An initial investigation of the association between the SARS outbreak and weather: with the view of the environmental temperature and its variation. J. Epidemiol. Community Health 59, 186–192.
Vandini, S., Corvaglia, L., Alessandroni, R., Aquilano, G.,Marsico, C., Spinelli, M., et al., (2013).Respiratory syncytial virus infection in infants and correlation with meteorological factors and air pollutants. Ital. J. Pediatr. 39(1).
Wang, Y.,Wang, Y., Chen, Y., Qin, Q., (2020b) Unique epidemiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID-19) implicate special control measures. J. Med. Virol.
Widiarso T. Rekayasa Gaya Hidup Menuju Kota Masa Depan Yang Berkelanjutan Di Indonesia. Yuan, J., Yun,H., Lan, W.,Wang, W., Sullivan, S.G., Jia, S., et al., (2006) A climatologic investigation of the SARS-CoV outbreak in Beijing, China. Am. J. Infect. Control 34, 234–236.
Zhu, N., Zhang, D.,Wang,W., Li, X., Yang, B., Song, J., et al., (2019) A novel coronavirus from patients with pneumonia in China. N. Engl. J. Med.
Biographies

Prayas Sharma is currently working as Assistant Professor in the area of Decision Sciences at Indian Institute of Management Sirmaur, Paonta Sahib, Himachal Pradesh. He has more than 9 years of academic experience, both in the domain of teaching and research. His research interest includes Survey Sampling, Estimation Procedures using Auxiliary Information and Measurement Errors, Predictive Modelling, Business Analytics and Operations Research. Dr. Sharma has published more than 40 research papers in reputed National & International journals along with one book and two chapters in book internationally published. He has more than 300 citations with H-Index & I index of 12. Dr. Sharma has a keen interest in reading, writing and publishing, he is serving 7 reputed journals as editor/associate editor and more than 30 journals as reviewer and reviewed more than 150 research papers from the prestigious journals.

Nitesh Kumar Adichwal is currently working as Assistant Professor in the School of Business, UPES, Dehradun. He has published several papers in the indexed journals in the field of sampling, Management and Demography. He is serving as reviewers for several good journals.

Ashish Kumar Singh currently working at Department of Management Studies, Raj Kumar Goel Institute of Technology, Ghaziabad. He has more than ten years of academic experience in management education and gives training at statistical tools with hands-one exercises. Apart from Ph.D. in Business Management he is having Executive Certificate in Business Analytics and Big Data from Indian Institute of Management (IIM)KASHIPUR & Certificate in “Data Science: R Basics” from Harvard University, Massachusetts Hall Cambridge, MA. He has contributed number of research papers and articles in various national and international journals indexed in Scopus (Elsevier) index, Web of Science (Clarivate Analytics), ABDC Category.
Journal of Reliability and Statistical Studies, Vol. 15, Issue 2 (2022), 535–552.
doi: 10.13052/jrss0974-8024.1526
© 2022 River Publishers