Effectiveness of the VR Cognitive Training for Symptom Relief in Patients with ADHD
Seok Hee Oh1, Jung Woon Park1 and Seong-Jin Cho2,*
1Gachon University, Seongnam, South Korea
2Gachon University College of Medicine, Incheon, South Korea
E-mail: seokhee5@gachon.ac.kr; pjw0129@gc.gachon.ac.kr; sjcho@gachon.ac.kr
Corresponding Author
Received 29 October 2021; Accepted 22 December 2021; Publication 08 March 2022
Abstract
This study aimed to verify the effectiveness of virtual reality (VR) cognitive training by measuring the sense of presence and electroencephalography (EEG) in children with ADHD. A clinical trial was conducted to verify the effect of VR cognitive training on children with ADHD. The experimental group included eight children with ADHD, and the control group included eight healthy children without ADHD. The sense of presence increased significantly after the VR cognitive training in children with ADHD. Also, no significant changes in the alpha, beta, delta, and gamma wave amplitudes were found in both groups after the VR cognitive training. Thus, the VR training content developed in this study can help measure the patients’ behavioral inhibition, increase their sense of presence by inducing interaction with distraction stimuli, and alleviate their symptoms. However, EEG could only be used as an auxiliary means, at the clinician’s judgment, for ADHD diagnosis in children because no significant EEG changes were observed in the experimental or control groups after the VR cognitive training.
Keywords: Virtual reality, ADHD, sense of presence, VR cognitive training, EEG, game engine.
1 Introduction
The proportion of children with attention deficit hyperactivity disorder (ADHD) increased sharply in South Korea [1] due to adverse effects of early years education and various environmental factors. Thus, interest in various therapies to treat ADHD at an early stage increased [2].
ADHD is one of the most common mental disorders in children. It is a chronically progressing psychiatric disorder that develops in early childhood [3]. Its major symptoms include being easily distracted, hyperactivity, impulsiveness, and learning disabilities. Negative symptoms such as carelessness, hyperactivity, and impulsiveness may continue into adulthood if children with ADHD are not treated early. These symptoms could lead to social disabilities that affect learning, employment, marriage, and health. Thus, there is an urgent need for early treatment [4–7].
Various methods are used to treat ADHD. ADHD treatments are primarily divided into pharmacologic treatments such as psychostimulants and non-pharmacologic treatments such as counseling and behavioral therapy [8, 9]. However, research on non-pharmacologic treatments in South Korea attracts more attention because most Korean parents do not perceive children with ADHD as having a disorder and are reluctant to use pharmacologic treatments, leading to treatment de-lays [10, 11]. Also, the importance of non-pharmacologic treatments is increasingly emphasized because pharmacologic treatments are limited. Moreover, therapeutic effects increase when both treatment types are combined, particularly when pharmaco-logic treatments are complemented by psychosocial therapies, such as cognitive behavioral therapy. Although pharmacologic treatments can reduce negative attitudes or unstable emotional states, they are limited in inducing correct behavioral response patterns [12, 13]. On the other hand, psychological therapies and behavioral interventions effectively prevent secondary problems [2].
Behavioral interventions and psychological therapies, including cognitive training, behavioral parent training (BPT), and social skills training programs, are recommended for children with ADHD [11]. Among these methods, many researchers focus on cognitive training using virtual reality (VR) content developed for educational and clinical environments because VR content motivates people undergoing training and provides dynamic testing and training situations [14–16].
In the cognitive training method using VR content, an artificial 3D environment is created utilizing computer technologies. A head mounted display (HMD)—a wearable VR device—tracks the wearer’s head movements to create a sensation of movement through a simulated 3D environment [17]. The VR experience using the HMD is more than passive acceptance of an image on an external screen [18]. In particular, VR games make possible immediate and continuous interaction [19]. VR enables users to make otherwise unavailable choices and creates positive changes in the users by strengthening their motivation to participate based on having fun and immersing themselves in a virtual reality environment (VRE) [20]. Thus, VR content provides a training environment that meets ADHD patients’ needs as a result of interaction based on hu-man-computer interface and immersion characteristics [21].
In general, children with ADHD are characterized by speaking or acting in ways incompatible with a situation and the inability to focus on a given task [4]. During training using VR content, children with ADHD are surrounded by a VRE. Their immersion is increased by the illusion that they share the same physical space, resulting in the sense of purpose that promotes participation and attention [23]. A VRE can enhance a sense of presence more than the existing PC-based or textbook-based counseling and training treatments [15]. The sense of presence is a sense of being in a specific place (a sense of being there), even while being in a different place physically [24]. Also, re-searchers found that a VRE has fewer ethical issues than the exposure-based therapy used in the actual clinical field for children with ADHD, who are subjected to negative feedback for their low attention span [20].
An increased number of studies validate VR cognitive training as a highly effective ADHD treatment [25]. These studies are supported by the evidence from electroencephalography (EEG) and an improved sense of presence in ADHD patients and pro-vide scientific justification for the usefulness of VR as an ADHD treatment. Thus, the analysis of the effectiveness of VR cognitive training is possible based on the EEG and improved sense of presence data obtained in the treatment process. Accordingly, this study will verify the VR cognitive training effectiveness based on the EEG and sense of presence analysis.
Various cognitive training methods to increase attention and the sense of presence in children with ADHD through behavioral inhibition training were attempted [4]. Previous studies revealed that most children with ADHD exhibit a low sense of presence due to weak motivation and poor concentration when learning. Thus, cognitive training to increase the sense of presence should focus on a highly realistic user experience, encourage user participation and ensure the completion of an activity. Such training can bring about changes in user behavior [26, 27].
The sense of presence could be affected by vividness and interaction [28]. In the end, to increase the sense of presence in a VRE, subjective sensations that come alive through interaction [27] and a subjective sense of vivid movement are important [6]. For example, a study on Finnish teenagers in 2005 highlighted interaction in a virtual environment [29]. The participants stated that the main difference between games and novels and movies was in the interactivity of games. In games, the teenagers made decisions, took actions, and exercised influence [30]. Another study argued that the sense of presence is at the core of a computer game experience due to the interactive nature of games [31]. Above all, due to changes in a VRE and interaction with the user’s HMD rotation and body movements, VR can increase the sense of presence and, therefore, training effectiveness. This proves that a VR strategy is effective in ADHD patients. VR, similar to real life, improves the user’s sense of presence while increasing the realism of tasks and activities, helping the user recognize and understand problems [32].
A VR therapy provides a topic and motivates children with ADHD to participate in active treatment [33]. Furthermore, researchers can safely control clinical trials and measure the results objectively by providing real-world conditions in a rigorous virtual environment [34]. For these reasons, VR received much attention from researchers and is used as an evaluation and cognitive training tool for patients with ADHD [22].
The importance of EEG in the process of VR cognitive training is explained below. EEG was the first measurement method to examine the brain’s cortical activity systematically [35]. Hans Berger first reported the use of EEG technology in the 1920s. These days, EEG is used to study children who are highly likely to be diagnosed with ADHD [36]. The frequency bands of interest in the study of ADHD are alpha, beta, gamma, and theta. Normalization of the corresponding EEG frequencies indicates a relief of ADHD symptoms.
Active research was conducted on EEG as a neurobiological index of ADHD [37, 38]. Typical EEG markers observed in patients with ADHD are increased theta power and reduced alpha and beta power in the frontal and central regions [39]. The most extensive EEG study on ADHD reported an increase in the theta wave activity, a slight increase in the frontal alpha wave activity, and a diffused decrease in the mean beta frequency in children with ADHD [38]. A VRE resembles an actual environment, and the user is provided with a direct experience in a virtual space that does not exist in reality [40]. In that situation, EEG can be used to analyze the user’s emotions and biometric data scientifically. Thus, the number of studies using EEG to analyze VR experience increases [41].
However, despite the findings presented above, using VR to treat children with ADHD is still limited. Specifically, utilizing VR content as a cognitive training tool for children with ADHD is limited because using VR content for extended periods is difficult, as children with ADHD are easily distracted and less focused. Also, the use is partially restricted due to VR devices’ characteristics. For example, the HMD might be too heavy, and physical discomforts such as nausea, dizziness, cybersickness, and eye fatigue may occur following sensory mismatch when a VR device is used for a long time [42, 43]. Therefore, to produce more useful and comfortable VR content that can be used as a treatment tool for children with ADHD, in this study, we developed a high-quality VR program that generates fun and interest in the cognitive training process and enables continuous and repetitive training based on the Unreal game engine technology.
This study seeks to apply the developed program for children with ADHD and investigate the effect of VR content as a cognitive training tool. To this end, this re-search intends to utilize the high-quality VR program to conduct a clinical trial on the effects of VR content on children with ADHD, centering on the variables mentioned above, namely, the sense of presence and EEG. At present, few studies attempted to verify the effect of VR content on children with ADHD in South Korea. Customized treatment interventions based on symptoms may be planned for children with ADHD by considering the EEG measurements and the sense of presence while using VR. The moderating effect of cognitive training could also be expected.
2 Materials and Methods
2.1 Research Participants
A clinical trial was conducted to verify the effect of VR content developed by the researchers in this study on ADHD patients. However, it was difficult to establish a control group in a short period of time as this study was also a pilot study. Therefore, one of the limitations of this study is the absence of the ADHD control group.
We intended to form an experimental group of at least 30 participants. However, there were difficulties in coordinating the clinical schedules of the patient and control groups. Therefore, with the approval of the IRB committee, we recruited ADHD patients and healthy participants treated at Gil Hospital, Samsung Medical Center, and Inha University Hospital in South Korea for the clinical trial.
Since ADHD symptoms mainly appear in children first, we limited the recruitment to elementary school students aged 8 to 13 years (1–6th grades). The experimental group included eight ADHD patients, and the control group included eight healthy participants without ADHD. The clinical trial was conducted at the VR Cognitive Training Center of Gil Hospital, Samsung Medical Center, and Inha University Hospital in South Korea from June 2018 to December 2019. The children in the experimental group were diagnosed with ADHD by a psychiatrist. They were capable of making decisions, continued receiving medicine and psychotherapy for more than one month, and had stable mental health symptoms (CGI score 4). Table 1 describes the general characteristics of the participants.
Table 1 Participants’ characteristics
| Gender | Mean Age | Mean | Mean | |||
| N | Group | M | F | (Years) | Height (cm) | Weight (kg) |
| 16 | Control | 5 | 3 | 8.5 | 130.9 | 27.8 |
| Experimental | 1 | 7 | 9 | 137.1 | 34.1 | |
| Note. N total number of the participants; M male; F female. |

Figure 1 VR cognitive training places for ADHD patients. (a) VR cognitive training center at Gil Hospital; (b) Samsung Medical Center; (c) Inha University Hospital.
2.2 Compliance with Research Ethics
This study implemented the following procedures and consent processes to ensure the research participants’ safety and compliance with bioethics. First, children participating in the study and their parents were provided with an explanation of the study’s purpose and aim and notified that the collected data would only be used for research purposes. Moreover, they were also informed that they could discontinue participating in the study at any time if they felt burdened by having to participate or had doubts about the research process. In particular, participants’ safety was emphasized, and the participants were guaranteed that no adverse effects or risks resulted from participating in the study.
Second, the study participants (parents and children) were given a written ex-planation of the study and written informed consent was obtained from each participant. Finally, the institutional review board’s approval (IRB: GAIRB2018-052) was received on February 13, 2018, from the clinical research ethics review committee of Gachon University Gil Medical Center.
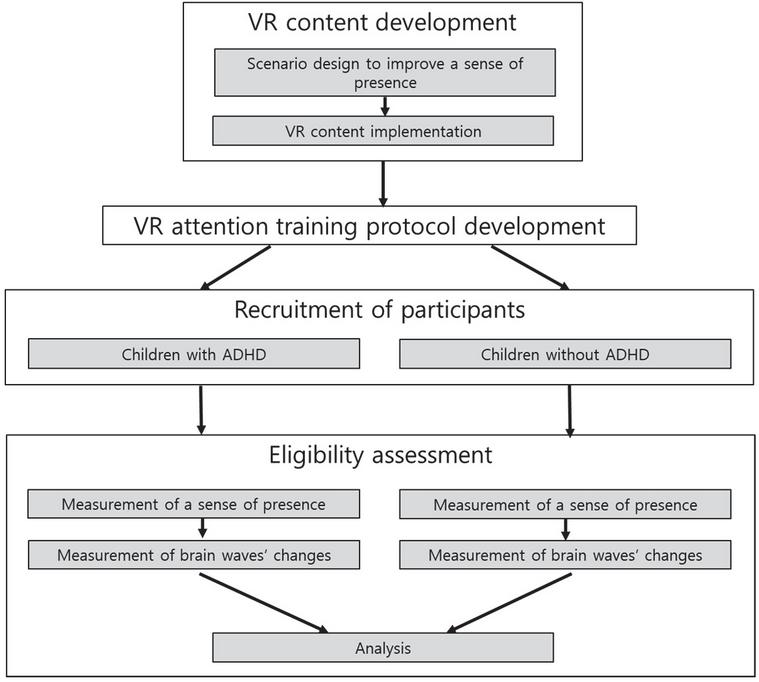
Figure 2 Research procedures flowchart.
2.3 Research Procedures
This study followed the procedures outlined in Figure 2 to achieve its purposes. Samsung Odyssey HMD was used in the study’s clinical trial. All research participants sat on a chair and proceeded with the experiment by using controllers. During the experiment, each hospital’s clinical psychologist explained the questionnaire, experimental method, and use of the VR HMD. The clinical psychologists also helped the participants to put on the HMD and EEG sensors.
This clinical trial was carried out over eight sessions, and the scores reflecting the correct or incorrect answers in each screening test were recorded in a log format and sent to a database. These data were used for the 2.2.5 VR Content Evaluation Index development by analyzing the sense of presence relationship surveyed through a questionnaire and the sense of presence relationship based on the EEG signals.
2.4 VR Cognitive Training Content Design
In this study, to verify the therapeutic effects of VR content on children with ADHD, a VR content scenario was designed based on the Advanced Test of Attention (ATA). The ATA is a newly developed test for ADHD diagnosis. It measures the individual’s perceptual tracking ability; psychomotor speed; sequential processing ability; verbal, visual, and auditory memory; attention; and concentration.
The VR content scenario was designed to enhance behavioral inhibition. Thus, the intention was for the participants to perform tasks to develop behavioral inhibition in a designed VRE. Furthermore, considering that the participants were children, the content with a rollercoaster VR concept was designed. The participants followed the directions and shot targets while riding a VR outdoor rollercoaster.
2.5 Scenario Development
The purpose of the VR content produced in this study was to conduct clinical trials in patients diagnosed with ADHD and verify its effectiveness. For this purpose, the study participants were selected based on the criteria outlined in Table 2 and psychiatrists’ and clinical trial experts’ advice.
Table 2 Participants’ inclusion and exclusion criteria
| Inclusion Criteria | Exclusion Criteria |
| Individuals capable of making decisions Individuals diagnosed with ADHD by a psychiatrist based on DSM-5 Individuals who continued to receive medicine and psychotherapy for more than a month Individuals with stable mental health symptoms (CGI score 4) | Individuals incapable of communication Individuals with severe medical disease Individuals with organic mental disorders Individuals with intellectual disabilities Individuals with an autism spectrum disorder Individuals with acute psychotic symptoms Individuals with major neurocognitive disorders Individuals with severe psychiatric symptoms (CGI-S score 5) |
| Note. DSM–5 Diagnostic and Statistical Manual of Mental Disorders (DSM–5) (2013). | |
The designed VRE included various objects and virtual avatars as distraction stimuli to measure behavioral inhibition. An outdoor train ride scenario was modified to include gamification components and reproduced in a rollercoaster format. Before the game started, the participants selected the time for each stage ranging from 10 to 50 seconds. The behavioral inhibition training presented distraction stimuli other than objects that met the conditions. In the process, positive responses, omission errors, and false alarm errors were measured.
The participants were provided with the following instructions on how to participate in the VR activity: Now, let’s start attention training outdoors. Riding the rollercoaster, you will see a zebra, giraffe, dolphin, duck, and spaceship balloons. When you hear a ‘ding-dong’ sound and an announcement, pay close attention. Follow the directions given in the announcement and pop a balloon with your gun. Be careful not to pop a balloon that does not fit the description given in the announcement. Also, be careful not to shoot rocks, trees, moving birds, butterflies.

Figure 3 Behavioral inhibition VR rollercoaster activity images. (a) VR content for ADHD training; (b) VR play scene; (c) zebra, giraffe, dolphin, duck, and spaceship-shaped balloons.
2.6 VR Cognitive Training Content Development
We used Unreal game engine 4 developed by Epic Games, Inc. for the VR content implementation. The Unreal engine is written in the C programming language and has high-quality live-action graphic expressiveness. In addition to games, it is used in various interaction videos and simulation fields.
The Odyssey VR HMD device by Samsung was used to demonstrate the VR content because it does not cause inconvenience to those wearing glasses and enables experience without installing separate sensors.

Figure 4 Examples of the VR cognitive training’s user interface for patients with ADHD. (a) A game/training scenario selection appears in the content pane, including concentration training and cognitive training. (b) Detailed difficulty levels appear after a game/training scenario is selected. (c) A user rides a VR rollercoaster when the outdoor activity is selected.

Figure 5 Examples of the VR content for patients with ADHD. (a) The user follows the directions and grabs balloons on the left and right using the controller. (b) The user listens to the directions until the rollercoaster game is over and continues with a balloon-grabbing game.
2.7 Program Protocol Development
A protocol was developed to increase executive functions, memory, and attention of patients with ADHD for the outdoor game content. To this end, the VR content was developed based on the existing ATA and the Stroop Color-Word Test (Stroop test).
The ATA is an evaluation program that measures continuous and selective attention and impulse suppression in children and adolescents using a computer [44]. The Stroop test is a neuropsychological test developed to evaluate the effectiveness of the inhibitory processes controlled by the frontal lobe [45]. The Stroop test assesses auto-mated response inhibition. During the test, the participants are asked to name the word’s color when the ink color and the color denoted by the word do not match [44]. Slow responses are known to reflect the inhibitory processes in the frontal lobe. A standardized study conducted in South Korea using the Stroop test found that the frontal lobe’s inhibitory functions were lower in children with ADHD than in children not diagnosed with ADHD.
Table 3 presents the program’s introduction and information on the VR device and training goals provided to the participants before the training.
Table 3 Attention training program protocol for patients with ADHD using virtual reality
| Session 1 | Sessions 2–7 | Session 8 |
|
1. Introduction of the attention training program 2. Instruction about the controller usage 3. Setting the goal for the session 4. Attention training using VR 5. Conclusion of the session |
6. Introduction of the attention training program 7. Review of lifestyle after the previous session 8. Instruction about the controller usage 9. Setting the goal for the session 10. Attention training using VR 11. Conclusion of the session |
1. Introduction of the attention training program 2. Review of lifestyle after the previous session 3. Instruction about the con-troller usage 4. Setting the goal for the session 5. Attention training using VR 6. Conclusion of the session 7. Review of the subject’s progress 8. Review of acquired skills 9. Conclusion of the entire program |
Table 4 ADHD VR content evaluation indicators
| Questionnaire | Biometric Data Items | |||
| and | Therapeutic | Evaluation of the | ||
| Evaluation Tool | Category | Diagnosis | Effect | VR Content |
| Korean version of the Conners Adult ADHD Rating Scale-IV Rating Scale-26 (K-CAARS -26) | EEG |
• Increase in delta wave activity • Increase in theta wave activity (frontal lobe, particularly) • Decrease in alpha wave activity • Decrease in beta wave activity • Increase of low-frequency activation • Increase in slow-wave activity in the frontal lobe |
• Normalization of delta wave activity • Normalization of theta wave activity • Normalization of alpha wave activity • Normalization of beta wave activity • Normalization of slow-wave activity in the frontal lobe |
• Sense of presence • Safety (motion sickness) evaluation • Convenience of use • Training convenience • Satisfaction • Matters to improve |
2.8 Program Protocol Development
2.8.1 Height and Weight
To measure the participants’ basic fitness, they were asked to fast for one hour before measurements were taken and participate in ADHD training sessions wearing light clothing, such as short-sleeved tops and shorts. The participants’ height (cm) and weight (kg) were measured and recorded. The general characteristics of the study participants were identified by examining their physical condition according to the demographic information criteria that could determine their health status.
2.8.2 Sense of Presence
The study measured the sense of presence in the control group (individuals not diagnosed with ADHD) and the experimental group (individuals diagnosed with ADHD) to verify the effect of VR content in cognitive terms. The measurements were taken by having the participants respond to a questionnaire based on the sense of presence scale developed by Witmer and Singer [46, 47]. The scale was adapted to suit the VRE of the current study. The questionnaire included 18 items measured on a 10-point Likert scale.
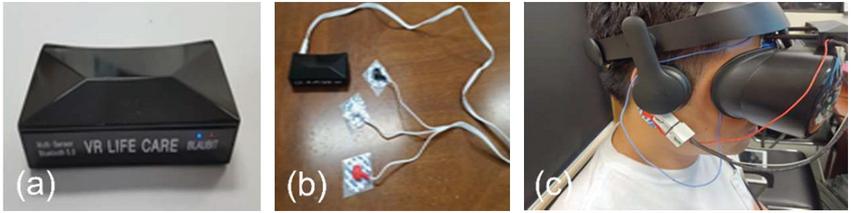
Figure 6 Composite biometric sensor terminals with EEG and PPG(photoplethysmography) data extraction and transmission functions. (a) sensor device 1; (b) sensor device 2; (c) sensor head mounting device.
2.8.3 EEG
EEG measurements were taken to verify the effect of VR content on physiological characteristics. Measurements were taken by using the EEG and PPG devices (Figure 6). Also, alpha, beta, delta, gamma, and theta waves were measured. The EEG measuring device utilized two channels and was attached to the forehead to measure the frontal lobe EEG. The technician in charge of the EEG measurements designed the biometric data analysis program and applied the machine learning SVM(Support Vector Ma-chine) to classify the data. Table 5 outlines sensor devices’ specifications.
Electrical flow is generated when signals are transmitted between cranial nerves in the nervous system. This neurophysiological measurement of the electrical activity of the brain is recorded through electrodes attached to the scalp. The EEG recordings demonstrate complex patterns, and the wave frequency bands are arbitrarily classified as delta, theta, alpha, beta, and gamma (Table 6).
Table 5 Sensor devices’ specifications
| Item | Specification |
| Sampling rate | 512 Hz |
| Resolution | 12Bit ADC, 1mV pk-pk EEG max, signal input |
| Operation voltage | 2.97 V–3.63 V |
| Hardware filtering | 3 Hz–100 Hz |
| Output the original EEG signal | Including connection, relaxation |
| Brain waves | Delta, theta, low-alpha, high-alpha, low-beta, high-beta, low-gamma, mid-gamma |
Table 6 Brain waves’ classification
| Type | Frequency Band (Hz) | Description |
| Delta | 0.5–4 | These are mainly measured in a state of deep sleep. A strong reaction occurs in the scalp. |
| Theta | 4–8 | These waves do not appear well in adults and are characterized by a serrated amplitude. They are mainly measured in an emotional state or cognitive state. They may be pathologically linked to the slowing of the alpha waves. |
| Alpha | 8–13 | These are measured when a person is awake. A strong reaction occurs in the occipital region. These are best measured when the person’s eyes are closed, or the person is relaxed, and activity is blocked or attenuated when mental efforts, such as visual attention, are made. |
| Beta | 13–30 | These indicate increased alertness and concentration. |
| Gamma | 30 | The gamma activity is linked to information processing (e.g., recognition of sensory stimuli)—spontaneous movement, related to information processing speed in the brain. |
2.9 Data Analysis
Our study’s data were analyzed with the SPSS software (Version 25, SPSS Inc, IL, USA), and mean and standard deviation were calculated. First, the Shapiro-Wilk normality test was conducted. After that, a paired t-test and Wilcoxon’s Signed Rank Test were performed to check the changes in the sense of presence and EEG of the ADHD group and control group before and after the VR cognitive training. For inter-pretation of analysis results, the significance level () was set to 0.05.
3 Result
3.1 Sense of Presence
Table 7 shows the changes in the sense of presence of the ADHD and control groups after the VR cognitive training. The sense of presence changed significantly after the VR cognitive training in the ADHD group . However, there were no such changes in the control group after the VR cognitive training.
Table 7 Changes in the sense of presence after the VR cognitive training
| Group | Before Training | After Training | ||
| ADHD | 116.63 30.65 | 120.13 29.40 | 2.90 | 0.02 |
| Control | 111.88 27.39 | 105.63 25.38 | 0.53 | 0.62 |
| ***. |
3.2 EEG
This study is meaningful as a pilot study investigating the relationship between VR treatment and EEG. Verification of normality was performed in the statistical analysis process. The data whose normality was verified was denoted by t. We also performed nonparametric tests for different data. Thus, t and z were written together in the results. Table 8 presents EEG changes (alpha, beta, delta, gamma, and theta waves’ amplitudes) in the ADHD and control groups after the VR cognitive training. After the VR cognitive training, there were no significant alpha, beta, delta, or gamma wave activity changes in both groups.
Table 8 EEG changes after the VR cognitive training
| Wave | Group | Before Training | After Training | ||
| Alpha | ADHD | 6.93 2.04 | 7.88 1.83 | 1.38 | 0.21 |
| Control | 8.79 0.93 | 9.14 0.66 | 1.38 | 0.21 | |
| Beta | ADHD | 6.75 2.14 | 7.00 1.62 | 0.28 | 0.78 |
| Control | 7.87 1.19 | 7.15 1.10 | 1.92 | 0.10 | |
| Delta | ADHD | 3.37 1.21 | 3.53 1.34 | 0.80 | 0.45 |
| Control | 3.40 1.13 | 3.90 1.16 | 1.26 | 0.25 | |
| Gamma | ADHD | 5.41 2.13 | 5.44 1.38 | 0.98 | 0.33 |
| Control | 6.00 1.62 | 5.08 1.21 | 1.55 | 0.16 | |
| Theta | ADHD | 10.05 2.27 | 9.72 2.16 | 0.67 | 0.53 |
| Control | 7.73 2.68 | 8.40 2.51 | 0.69 | 0.51 | |
| ***. |
4 Discussion
This study investigated the effects of VR content as a training tool on relieving ADHD symptoms in children. The developed VR cognitive training was implemented for the ADHD and control groups of children to this end. Changes in the sense of presence and EEG after the VR cognitive training are as follows. First, the sense of presence in the ADHD group increased after the VR cognitive training. However, no significant difference was found in the control group after the VR cognitive training. The results suggest that the VR cognitive training could increase the sense of presence, which signifies the relief of ADHD symptoms in cognitive terms. The results point to the possibility of using VR cognitive training to treat patients with cognitive or behavioral disorders such as ADHD or other mental disorders. Since people suffering from mental health issues are aware that a VRE is a computer-fabricated environment, they can respond to challenging situations that they avoided in real life, thereby achieving new experiences and therapeutic effects [48].
The VR training content developed in this study can help measure the patients’ behavioral inhibition, increase their sense of presence by inducing interaction with distraction stimuli, and improve patients’ symptoms. This is consistent with the previous research that considered the sense of presence a core variable to increase the efficacy of ADHD cognitive training [49].
Second, no significant EEG differences were found between the ADHD and control groups after the VR cognitive training. In other words, the relief of ADHD symptoms after the VR cognitive training was not verified. A high activity level of the dormant delta and theta waves and a low activity level of the alpha and beta waves in children with ADHD, which were reported by previous studies, were not observed before or after the VR training in this study [39]. Considering previous research findings in South Korea that EEG is not an effective tool for ADHD diagnosis, the results of this study show EEG could be used as an auxiliary means, at the clinician’s judgment, for ADHD diagnosis in children.
This study is a pilot study. However, experiments, analysis, and verification over at least one year are required to obtain precise results versus this study’s 8-week cognitive training period. Nevertheless, the changes in the amplitudes of alpha, beta, delta, gamma, and theta waves in the experimental group after the VR cognitive training suggest its potential as an alternative treatment of ADHD. Furthermore, because the sample size in this study was small, with only eight ADHD cases considered, the results might be difficult to generalize, posing a question about their significance. In addition, this study did not have an ADHD control group, which is one more of its limitations.
In summary, the VR content developed in this study could be a viable non-pharmacologic treatment to help relieve ADHD symptoms in children. Game elements should be used to make the treatment more enjoyable, and interactive functions should motivate ADHD patients to participate in VR training [6, 50]. In the future, consultants who perform VR treatment can consult and treat more patients if evaluation and education in VR cognitive training are automated. Thus, the application of VR cognitive training is expected to expand, enabling the same professionals to consult and treat more patients and lower admissions to psychiatric departments, thereby helping to reduce the negative prejudices of the public [51].
Also, VR content can be utilized as an additional treatment means rather than a primary one. Considering that children enjoy games, it can be utilized as a selection tool to quickly and conveniently locate groups with the likelihood of ADHD. Consequently, VR cognitive training could help relieve ADHD symptoms, and its therapeutic effect is expected to grow as it can improve children’s concentration and immersion [12].
When psychosocial, cognitive therapy is merged with medication treatment, the effects of ADHD therapy can be maximized. Therefore, efforts should be made to develop and apply various types of VR content for children diagnosed with ADHD to increase their concentration and immersion in the therapy sessions [45].
Lastly, focusing on this study’s limitations, the researchers propose the following for constructive follow-up research. First, a long-term observational study should help to confirm the therapeutic effects of VR cognitive training on children with ADHD. Second, because most children who participated in this study were concurrently taking ADHD medication, follow-up research on the effects of VR cognitive training alone is required. Finally, from a national health perspective, developing methods and projects for VR cognitive training—a non-pharmacological treatment—of children with ADHD is of utmost importance to prevent the maladjustment of children with ADHD when they grow up.
Acknowledgments
This research was supported by the Ministry of Science and ICT (MSIT), Ko-rea, under the Information Technology Research Center (ITRC) support program (IITP-2021-2017-0-01630) supervised by the Institute for Information & communications Technology Promotion (IITP).
References
[1] National Health Insurance Service in Korea, ‘Eighty percent of all ADHD patients are male, and six out of ten are teenagers’, Jul., 2019.
[2] H. Cho, H. Jeong, ‘The effect of ROCF applied cognitive-behavioral art therapy on the performance of ROCF drawings by ADHD children and changes in major symptoms and problem behaviors’, The Journal of Cognitive Enhancement and Intervention, pp. 85–105, Korea, Nov., 2020.
[3] K. Ronald, et al., ‘The prevalence and correlates of adult ADHD in the United States: Results from the national comorbidity survey replication’, The American Journal of Psychiatry, pp. 716–723, Apr., 2006.
[4] W. David, M. Eric, ‘Behavioral and emotional disorders in adolescents: Nature, assessment, and treatment’, Guilford Press, pp. 3–20, Oct., 2006.
[5] B. Russell, et al., ‘The persistence of attention-deficit/hyperactivity disorder into young adulthood as a function of reporting source and definition of disorder’, Journal of Abnormal Psychology, pp. 279–289, Jun., 2002.
[6] S. Yeh, C. Tsai, Y. Fan, P. Liu, A. Rizzo, ‘An innovative ADHD assessment system using virtual reality’, IEEE-EMBS Conference on Biomedical Engineering and Sciences, Langkawi, 2012.
[7] P. Hurks, J. Hendriksen, ‘Retrospective and prospective time deficits in childhood ADHD: The effects of task modality, duration, and symptom dimensions’, Child Neuropsychology, pp. 34–50, Jun., 2010.
[8] S. Brown, ‘Method for diagnosis and treatment of psychological and emotional disorders using a microprocessor-based video game’, Google Patents, 1999.
[9] G. Park, ‘Time simulator in virtual reality for children with attention deficit hyperactivity disorder’, In: M. Herrlich, R. Malaka, M. Masuch (Eds.), Entertainment Computing – ICEC 2012, ICEC 2012, Lecture Notes in Computer Science Singapore, 2012.
[10] W. Park, S. Park, S. Hwang, ‘Effects of cognitive behavioral therapy on attention deficit hyperactivity disorder among school-aged children in Korea: A meta-analysis’, Journal of Korean Academy of Nursing, pp. 169–182, Apr., 2015.
[11] I. Y, G. Won, J. Kim, ‘Neurofeedback: Possibility of alternative non-pharmaceutical treatment for children with ADHD’, Journal of The Korean Society of Biological Therapies in Psychiatry, pp. 195–202, Aug., 2020.
[12] Y. Shin, et al., ‘The revised Korean practice parameter for the treatment of attention-deficit hyperactivity disorder (IV): Non-pharmacologic treatment’, J Korean Acad Child Adolesc Psychiatry, pp. 84–95, Mar., 2017.
[13] I. Kim, ‘The Effect of social skills training with attention-deficit hyperactivity disorder (ADHD)’, Korean Acad Psych Mental Health Nurs, pp. 420–428, Dec., 2007.
[14] J. Bailey, et al., ‘Virtual reality’s effect on children’s inhibitory control, social compliance, and sharing’, Journal of Applied Developmental Psychology, Jun., 2019.
[15] A. Rizzo, et al., ‘A virtual reality scenario for all seasons: the virtual classroom’, CNS Spectrums, pp. 35–44, Nov., 2014.
[16] B. Azadeh, et al., ‘The opportunities of virtual reality in the rehabilitation of children with attention deficit hyperactivity disorder: a literature review’, Korean Journal of Pediatrics, pp. 337, Nov., 2017.
[17] A, Karen, et al., ‘Virtual reality for pain and anxiety management in children’, Canadian Family Physician, pp. 932–934, Dec., 2017.
[18] P. Ali, et al., ‘Emerging utility of virtual reality as a multidisciplinary tool in clinical medicine’, Games for Health Journal, pp. 263–270, Oct., 2017.
[19] S. Nam, H. Yu, D. Shin, ‘User experience in virtual reality games: The effect of presence on enjoyment’, International Telecommunications Policy Review, pp. 85–125, Apr., 2021.
[20] C. Ryu, et al., ‘Effects of an anger management virtual reality cognitive behavioral therapy program on EEG patterns among destructive and impulse-control disorder patients’, Journal of Medical Imaging and Health Informatics, pp. 1319–1323, Sep., 2016.
[21] G. Burdea, P. Coiffet, ‘Virtual reality technology (2nd ed.)’, Wiley-IEEE Press, Jun., 2003.
[22] P. Yehuda, et al., ‘The utility of a continuous performance test embedded in virtual reality in measuring ADHD-related deficits’, Journal of Developmental & Behavioral Pediatrics, pp. 2–6, Feb., 2006.
[23] J. Blascovich, et al., ‘Immersive virtual environment technology as a methodological tool for social psychology’, Psychological Inquiry, pp. 103–124, Aug., 2002.
[24] H. Carrie, ‘Communication research on consumer VR. Communication in the age of virtual reality (1st ed.)’, Routledge, pp. 191–218, Mar., 1995.
[25] J. Park, et al., ‘Design and implementation of VR-based life care contents for attention deficit hyperactivity disorder (ADHD)’, The Journal of Korean Institute of Next Generation Computing, pp. 84–91, Oct., 2019.
[26] R. Giuseppe, et al., ‘The VEPSY updated project: virtual reality in clinical psychology’, Cyber Psychology & Behavior, pp. 449–455, Jan., 2001.
[27] S. Yeon, C. Ryu, ‘Recent developments of anger management virtual reality cognitive behavioral therapy [VR-CBT] program for juvenile offenders’, Korean Institute of Criminology, pp. 1–102, Dec., 2015.
[28] S, Jonathan, ‘Defining virtual reality: Dimensions determining telepresence’, Journal of Communication, pp. 73–93. Jul., 2006.
[29] C. Ryu, ‘Implications of developmental tasks of anger management virtual reality therapy techniques based on bio-signal pattern analysis for ADHD in adolescents and adults: Focused on crime prevention and inhibition skills for violence with unspecified motivation against strangers’, Korean Association of Addiction Crime Review, pp. 43–73, Jul., 2018.
[30] E. Laura, ‘Fundamental components of the gameplay experience: Analysing immersion’, DiGRA 2005 Conference: Changing Views – Worlds in Play, pp. 37–53, June., 2005.
[31] Y. So, ‘A Comparison analysis of usability evaluation for simulation learning based on web 3D and virtual reality’, The Journal of the Korea Contents Association, pp. 719–729, Aug., 2016.
[32] B. Wilson, K. M. Myers, ‘Situated cognition in theoretical and practical context. In D. H. Jonassen & S. M. Land (Eds.)’, Theoretical foundations of learning environments, pp. 57–88, Nov., 2009.
[33] A. Rizzo, et al., ‘Virtual environment applications in clinical neuropsychology’, Proceedings IEEE Virtual Reality 2000 (Cat. No. 00CB37048), pp. 63–70, Mar., 2020.
[34] F. Mantovani, G, Castelnuovo, ‘The sense of presence in virtual training: Enhancing skills acquisition and transfer of knowledge through learning experience in virtual environments. In Being There: Concepts, effects and measurement of user presence in synthetic environments; (Eds.)’, Ios Press, pp. 167–182, Oct., 2003.
[35] S. Loo, S. Makeig, ‘Clinical utility of EEG in attention-deficit/hyperactivity disorder: a research update’, Neurotherapeutics, pp. 569–587, Jul., 2012.
[36] B. Hans, ‘On the electroencephalogram of man’, Electroencephalogr Clin Neurophysiol, 1969.
[37] S. Oh, et al., ‘Association between quantitative electroencephalography findings and cognitive-behavioral characteristics in attention deficit/hyperactivity disorder: a retrospective cross-sectional study’, Journal of Korean Neuropsychiatric Association, pp. 266–273, Aug., 2018.
[38] R. Chabot, et al., ‘Sensitivity and specificity of QEEG in children with attention deficit or specific developmental learning disorders’, Clinical EEG and Neuroscience, pp. 26–34, Jan., 1996.
[39] R. Barry, A. Clarke, S. Johnstone, ‘A review of electrophysiology in attention-deficit/hyperactivity disorder: I. Qualitative and quantitative electroencephalography’, Clinical Neurophysiology, pp. 171–183, Feb., 2003.
[40] C. Lee, ‘Digital therapeutics using brain waves XR research on how to create contents’, The Korean Journal of Animation, pp. 197–209, Dec., 2020.
[41] J. Park, et al., ‘An analysis of the audience’s levels of emotion and immersion while watching short animated films using BCI & VR devices’, The HCI Society of Korea, pp. 765–768, Feb., 2019.
[42] S. Palmisano, R. Mursic, J. Kim, ‘Vection and cybersickness generated by head-and-display motion in the Oculus Rift’, Displays, pp. 1–8, Nov., 2016.
[43] K. Stanney, et al., ‘Cybersickness is not simulator sickness’, Proceedings of the Human Factors and Ergonomics Society Annual Meeting, pp. 1138–1142, Oct., 1997.
[44] M. Shin, M. Park, ‘A standardization study for the Korean version of the Stroop color-word test children‘s version’, Korean Psychological Association Annual Conference Program & Abstract, pp. 628–629, Oct., 2006.
[45] D. Frank, ‘The rise and fall of the inhibitory mechanism: Toward a unified theory of cognitive development and aging’, Developmental Review, pp. 45–75, Mar., 1990.
[46] B. Witmer, M. Singer, ‘Measuring presence in virtual environments: A presence questionnaire’, Presence: Teleoperators and Virtual Environments, pp. 225–240, Jun., 1998.
[47] H. Lee, et al., ‘The relationship between brain activities and presence on communication using an avatar in virtual reality’, Korean Journal of Cognitive Science, pp. 357–373, Mar., 2006.
[48] D. Frank, et al., ‘Virtual reality in the assessment, understanding, and treatment of mental health disorders’, Psychological Medicine, pp. 2393–2400, Mar., 2017.
[49] S. Thomas, et al., ‘The experience of presence: Factor analytic insights’, Presence: Teleoperators and Virtual Environments, pp. 266–281, Jun., 2001.
[50] T. Parsons, et al., ‘A controlled clinical comparison of attention performance in children with ADHD in a virtual reality classroom compared to standard neuropsychological methods’, Child Neuropsychology, pp. 363–381, Jun., 2007.
[51] D. Freeman, et al., ‘Automated psychological therapy using immersive virtual reality for treatment of fear of heights: a single-blind, parallel-group, randomised controlled trial’, The Lancet Psychiatry, pp. 625–632, Aug., 2018.
Biographies

Seok Hee Oh is an Associate Professor of Computer Engineering at Gachon University, Seongnam, South Korea. Oh received his Ph.D. degree in 2016 from the Department of IT Convergence Engineering, Gachon University Graduate School. He has worked at the Department of Computer Engineering, Gachon University, since 2016. Oh’s current and previous research interests include virtual reality, HCI, UX, and game design. He is a member of the Korea Game Society and the Gamification Forum.

Jung Woon Park is a Ph.D. candidate at the Department of IT Convergence Engineering, Gachon University, Seongnam, South Korea. Park received his Master’s Degree in Game Engineering in 2018 from the Department of IT Convergence Engineering, Gachon University Graduate School. He has worked on conceptual design and 3D modeling for game art since 2005. Park’s current and previous research interests include VR, metaverse, virtual production, and VFX. He is a member of the Korea Game Society.
Seong-Jin Cho is a Professor at the Department of Psychiatry, Gil Medical Center, Gachon University College of Medicine, Incheon, South Korea. Cho received his M.D, Ph.D. in 2004 from Seoul National University, College of Medicine, Seoul, South Korea. He has worked at the Department of Psychiatry, Gil Medical Center, Gachon University College of Medicine since 2000. Cho’s current and previous research interests include dementia, depression, and virtual reality. He is a member of the Korean Association of Geriatric Psychiatry, the Korean Neuropsychiatric Association, and the Korean Academy of Anxiety and Mood.
Journal of Web Engineering, Vol. 21_3, 767–788.
doi: 10.13052/jwe1540-9589.21310
© 2022 River Publishers